
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Suspected parathyroid carcinoma: Clinical diagnosis of unique endocrine pathology
Ashley Stutes, MD1*; Allison Tran2; David H Mull, MD1; Bernadette McLaren, MD3; Gazi Zibari, MD1; Donnie Aultman, MD1
1Willis Knighton Health System, USA.
2Edward Via College of Osteopathic Medicine, Blacksburg, Virginia, USA.
3Christus Health System, USA.
*Corresponding Author : Ashley Stutes
Willis Knighton Health System, USA
Email: astutes@wkhs.com &
stutesashley@gmail.com
Received : Jun 01, 2023
Accepted : Aug 18, 2023
Published : Aug 25, 2023
Archived : www.jcimcr.org
Copyright : © Stutes A (2023).
Abstract
Parathyroid carcinoma is an extremely rare malignancy of the endocrine system with an incidence of 0.5 - 5% of patients with hyperparathyroidism worldwide. It typically presents with an indolent course, and manifestations of hyperparathyroidism usually appear well before local invasion. However, here we will discuss the case of a 69-year-old male with parathyroid carcinoma who presented with a mass so large that it caused significant tracheal compression, dysphagia, and shortness of breath before it was correctly identified as parathyroid carcinoma. Diagnosis based on tissue specimen is particularly challenging, and the only absolute proof of malignancy is the presence of metastases. This is why diagnosis of this pathology is a largely clinical one, as was such in this case where pathology did not in fact identify the specimen as a malignancy, but it was certainly parathyroid carcinoma based on its overall clinical presentation.
Keywords: Parathyroid carcinoma; Hyperparathyroidism; Hypercalcemia; Airway compromise.
Abbreviations: PTH: Parathyroid hormone; CT: Computed Tomography
Citation: Stutes A, Tran A, Mull DH, McLaren B, Zibari G et al. Suspected parathyroid carcinoma: Clinical diagnosis of unique endocrine pathology. J Clin Images Med Case Rep. 2023; 4(8): 2561.
Introduction/background
Parathyroid carcinoma is a rare entity that typically presents initially with manifestations of hyperparathyroidism and has an overall indolent course. Men and women are equally affected, with disease occurring in the 4th or 5th decade of life [1]. Although the exact etiology is unknown, several genetic associations exist, including the mutation of the HPRT2 gene or those with multiple endocrine neoplasia syndromes. Patients typically present with symptoms of hypercalcemia such as fatigue, malaise, weakness, and weight loss [2]. Work up includes measurement of serum PTH and calcium as well as imaging studies including neck ultrasound and 99mTc-sestamibi scan. In suspected malignancy, a CT with contrast can provide specific details on the location of the lesion in relation to other structures. Though difficult to distinguish between the two, hypercalcemia symptoms are usually more pronounced in those with malignancy[3] (Table 1).
Management is divided into two categories, based on disease severity. Complete surgical excision may offer a definitive cure, with studies showing low efficacy of radiation and chemotherapy [4]. In patients with metastatic disease, medical management of hypercalcemia is recommended. Despite surgical efforts, parathyroid carcinomas have up to a 78% recurrence rate, most within the first 3 years.
Case presentation
69-year-old Caucasian male with past medical history of irritable bowel syndrome who presented to the ED with difficulty breathing and swallowing. Onset was 2 weeks prior, but symptoms had acutely worsened the night before. Patient endorsed throat pain that radiated to chest, neck, and head and that was exacerbated by coughing. He had a known history of a cystic neck mass which was previously drained and had since recurred. He reported an established history of hypercalcemia but no known diagnosis of hyperparathyroidism. His labs revealed a Calcium of 15.2 and PTH over 1400.
Table 1: Clinical factors of benign primary hyperparathyroidism and parathyroid carcinoma.
| Factor | Benign hyperparathyroidism | Parathyroid carcinoma |
|---|---|---|
| Sex distribution. F.M. frequency | 4:1 | 1:1 |
| Mean age at presentation, years | 55 | 48 |
| Serum calcium, mg/dl | < 13 | >14 |
| Serum parathyroid hormone | >1-3 X above the upper limit of normal | ≥ 4 X above the upper limit of normal |
| Palpable neck mass % | Rarely | 70 |
Table reproduced from Fingeret AL. Contemporary Evaluation and Management of Parathyroid Carcinoma. JCO Oncol Pract. 2021; 17(1): 17-21. doi: 10.1200/JOP.19.00540. Epub 2020 Feb 10. PMID: 32040373.
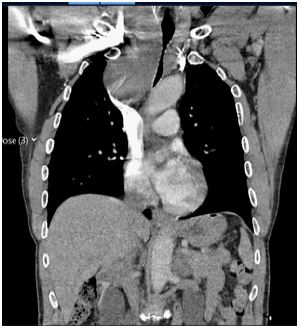
On physical exam, there was notable loud biphasic stridor. He also had secretions in the throat and grimaced when attempting to clear his throat. A neck and chest CT scan obtained revealed a large mass extending from the inferior margin of the right thyroid lobe through the thoracic inlet into the superior mediastinum producing severe mass effect (Figures 1&2). The mass measured at 10.4 x 7.7 x 12.6 cm with heterogeneity in the superior margin with internal cystic foci. There was severe narrowing of the subglottic trachea with lumen reduction to 8 x 6 mm and leftward tracheal displacement by 1-2 cm. The esophagus was also displaced to the left by 2-3 cm.
He ultimately underwent a parathyroidectomy and right thyroid lobectomy which was performed by Endocrine surgery and Cardiothoracic surgery, requiring a median sternotomy incision for full visualization. At the initiation of surgery, he required cardiopulmonary bypass as successful intubation was not able to be achieved due to such large mass effect on the trachea. He was successfully intubated further into the surgery once enough of the mass was able to be dissected off of the trachea. The mass was noted to be tightly adhered to the recurrent laryngeal nerve and appeared to be infiltrating surrounding soft tissues. Final specimens of the mass revealed the right lower neck component weighing 700 mg and the right mediastinal component weighing 1800 mg.

The final pathology was ultimately labeled as “atypical parathyroid tumor” and contained irregular proliferation of hypercellular parathyroid tissue that exhibited zones of fibrosis with hemosiderin deposition and calcification. Immunostaining was negative for malignancy markers including TTF1 (Thyroid transcription factor), thyroglobulin, & calcitonin. Additionally, atypical mitotic features were not appreciated, however invasion to the surrounding tissue and recurrent laryngeal nerve was noted. There was an absence of other typical malignant features including vascular invasion, perineural invasion, or elevated mitotic rate with atypical mitotic forms.
Discussion/conclusion
Parathyroid carcinoma is an extremely rare malignancy which can be difficult to distinguish from benign causes of primary hyperparathyroidism, particularly when it comes to pathological examination of tissue specimens. Pathological examination is described using a combination of mitotic figures, fibrous trabeculae, and capsular and vascular invasion as identifiers to point towards malignancy [3]. However, none of these criteria are sufficiently sensitive or specific to confirm or rule out diagnosis. Immunohistochemical staining has also been utilized but is not sufficient for accurate diagnosis either.
As pathological diagnosis is more ambiguous and less definitive, parathyroid carcinoma is a clinical diagnosis of which practitioners should be aware of. There are several presenting clinical features that are suggestive of malignancy rather than benign etiology. These include higher serum calcium levels and therefore more severe symptoms of hypercalcemia including fatigue, weakness, bone pain, nephrolithiasis, polyuria and polydipsia [4]. Remarkably elevated PTH levels are yet another indicator that points towards a diagnosis of malignancy. Grossly, these malignant tumors are usually quite large with an average diameter >3 cm and are often stubbornly adherent to surrounding structures, which lends itself to the fact that a palpable neck mass is far more common in these cases of malignancy rather than with benign etiologies [2].
With all of these factors in consideration, it is as such that in this case, while pathology reports identify the specimen as “atypical”, due to overall size, symptoms, and invasiveness, it is clinically deemed a parathyroid carcinoma.
Complete en bloc surgical excision remains the only treatment option that may offer a definitive cure, and even then, parathyroid carcinomas are noted to have recurrence rates of up to 78%, most often within the first three years [5].
Acknowledgements: The authors gratefully acknowledge the helpful discussions and overall guidance provided by Dr. Donnie Aultman and Dr. Krystle Trosclair.
References
- Mohebati A, Shaha A, Shah J. Parathyroid carcinoma: challenges in diagnosis and treatment. Hematol Oncol Clin North Am. 2012; 26(6): 1221-38. doi: 10.1016/j.hoc.2012.08.009. Epub 2012 Oct 5. PMID: 23116578
- Givi B, Shah JP. Parathyroid carcinoma. Clin Oncol (R Coll Radiol). 2010; 22(6): 498-507. doi: 10.1016/j.clon.2010.04.007. Epub 2010 May 26. PMID: 20510594; PMCID: PMC3781923.
- Shane E. Clinical review 122: Parathyroid carcinoma. J Clin Endocrinol Metab. 2001; 86(2): 485-93. doi: 10.1210/jcem.86.2.7207. PMID: 11157996.
- Busaidy NL, Jimenez C, Habra MA, Schultz PN, El-Naggar AK, Clayman GL, Asper JA, Diaz EM Jr, Evans DB, Gagel RF, Garden A, Hoff AO, Lee JE, Morrison WH, Rosenthal DI, Sherman SI, Sturgis EM, Waguespack SG, Weber RS, Wirfel K, Vassilopoulou-Sellin R. Parathyroid carcinoma: a 22-year experience. Head Neck. 2004; 26(8): 716-26. doi: 10.1002/hed.20049. PMID: 15287039.
- Hundahl SA, Fleming ID, Fremgen AM, Menck HR. Two hundred eighty-six cases of parathyroid carcinoma treated in the U.S. between 1985–1995: a National Cancer Data Base Report. The American College of Surgeons Commission on Cancer and the American Cancer Society. Cancer. 1999; 86:538–544. [PubMed: 10430265]
- Fingeret AL. Contemporary Evaluation and Management of Parathyroid Carcinoma. JCO Oncol Pract. 2021; 17(1): 17-21. doi: 10.1200/JOP.19.00540. Epub 2020 Feb 10. PMID: 32040373.