
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Delayed cerebral vasospasm following craniopharyngioma surgery: The impact of the electrolytes imbalance
Zahra Davoudi1; Guive Sharifi2; Saharnaz Ganjenejhad3; Sasan Alampour3; Zahra Jelokhani4; Yashar Goorakani5*
1Associate Professor, Department of Endocrinology, Skull Base Research Center of Loghman Hakim Hospital, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
2Associate Professor, Department of Neurosurgery, Skull Base Research Center of Loghman Hakim Hospital, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
3Department of Neurosurgery, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
4Qazvin Student Research Committee, Qazvin University of Medical Sciences, Qazvin, Iran.
5Department of Neurosurgery, Skull Base Research Center of Loghman Hakim Hospital, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
*Corresponding Author : Yashar Goorakani
Loghman-e-Hakim Hospital, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
Email: y.goorakani37@gmail.com
Received : Jun 19, 2023
Accepted : Aug 18, 2023
Published : Aug 25, 2023
Archived : www.jcimcr.org
Copyright : © Goorakani Y (2023).
Citation: Davoudi Z, Sharifi G, Ganjenejhad S, Alampour S, Goorakani Y, et al. Delayed cerebral vasospasm following craniopharyngioma surgery: The impact of the electrolytes imbalance. J Clin Images Med Case Rep. 2023; 4(8): 2562.
Introduction
Cerebral vasospasm is a well-known phenomenon following aneurysmal subarachnoid hemorrhage and trauma. While cerebral vasospasm is observed following skull base tumor surgery, it remains a rare phenomenon and is a major cause of neurologic morbidity and mortality [1,2].
To date, the main pathophysiology of vasospasm remains unclear but is thought vascular endothelial change is secondary to subarachnoid blood, the chemical effect of craniopharyngioma products, and fluid/electrolyte imbalance due to hypothalamic-pituitary axis instability [3,4].
Herein we report a case of delayed cerebral vasospasm following craniopharyngioma endoscopic transsphenoidal surgery; the possibility of Cerebral Salt Wasting Syndrome (CSWS) associated – stroke in this patient and a literature review regarding this dilemma has also been described in this manuscript.
Case report
A 14-year-old boy presented in the emergency room with low level of consciousness, 2 weeks after a transsphenoidal resection of a craniopharyngioma.
He was diagnosed with complaints of headache, diplopia, growth retardation, and delayed puberty and Magnetic Resonance Imaging (MRI) compatible with craniopharyngioma (Figure 1).
According to clinical and paraclinical data, Endoscopic TransSphenoidal Surgery (ETSS) was done.
There was no significant bleeding or vascular injury during surgery and with a stable post-operative state, but the patient’s neurologic status deteriorated with confusion and severe headache 2 days postoperative and the CT scan revealed hydrocephalous and he underwent ventriculoperitoneal shunting (Figure 2). During the hospital stay, he was under replacement therapy with prednisolone, levothyroxine, and DDAVP for diabetes insipidus. The patient was discharged on day 12 after surgery with stable symptoms and laboratory data.
Two days after discharge, the patient’s level of consciousness gradually decreased; He subsequently had irritability and loss of consciousness and was referred to Loghman-Hakim Hospital (Tertiary Center for pituitary surgery).
Physical examination revealed Blood pressure of 90/60, pulse rate of 100 /minute, GCS 10, and didn’t obey commands.
According to the history of recent surgery and following shunting our main primary impressions were electrolyte imbalance, meningitis, and increased ICP secondary to shunt malfunction; so related lab tests, brain CT; neurology consult was requested (Table 1, Figure 3a).
Laboratory results showed acute onset hyponatremia, that serum Na was 119 meq/l, random urine Na was 93 meq/l, and urine specific gravity: 1,023.
We started Antibiotics therapy (Meropenem and Vancomycin regimen for suspicious of meningitis); isotonic normal saline following hypertonic saline to maintain urine output and IV hydrocortisone for the primary impression of cerebral salt wasting or SIADH with acute adrenal insufficiency. He was transferred to ICU and electrolyte imbalance and anuria resolved. Following the early treatment, he presented with Diabetes insipidus (urine specific gravity: 1,007, urine production more than 500 cc/hour) and DDAVP started to control polyuria.
Despite all the initial treatment and support measures, the patient did not improve and presented with a decline in GCS and anisocoria, emergency CT demonstrated evidence of large left frontotemporoparietal hypodensity that infarction is our first impression with severe cerebral edema and <0.5 cm midline shift that reasonable for left internal carotid artery occlusion shown in figure 3b.
The emergency decompressive craniectomy was performed for the patient. The postoperative state was nearly favorable, so further diagnostic workups were performed to find the cause of the infarction; Carotid color Doppler sonography was remarkable and Brain MRI revealed restricted areas in the left cerebral hemisphere and right frontal lobe suggestive of recent ischemic infarction in left ICA and right ACA territories with hemorrhagic transformation with Evidence of SAH in prepontine cisterns (Figure 4).
Brain MR-Angiography reports multifocal moderate narrowing in the V4 segment of vertebral arteries, basilar artery, and PCAs, and also narrowing of the cavernosal segment of both ICAs more prominent on the left side, and multifocal moderate to severe narrowing in the left MCA; and also, cutoff A1 segment of both ICAs (Figure 5).
Cervical MR-Angiography documented that common carotid, cervical segments of vertebra arteries, internal and external carotid arteries also show normal appearance without any evidence of significant stenosis aneurysmal formation, or arterial occlusion in their arteries (Figure 6).
Finally, after 2 months of hospital stay, the patient was extubated and transferred to the ward with a stable condition and awake status but not obey and discharged from the hospital.
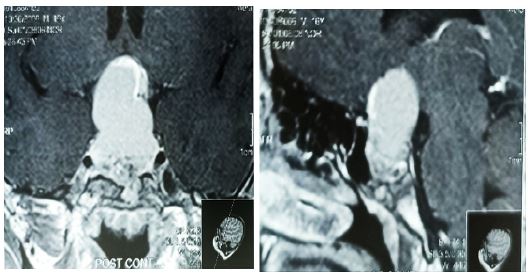

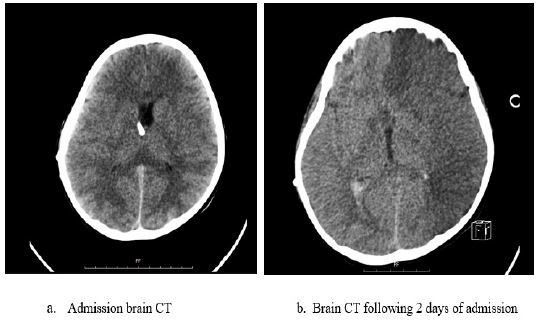
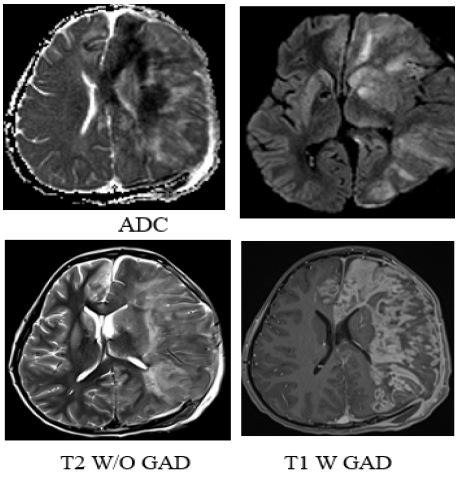


Table 1: Initial laboratory findings.
| WBC: 5.2 (4.8-10.8) Hb: 9.3 (13.5-17.5) Plt: 161 (140-450) BUN: 25 (18-45) Cr: 0.5 (0.5-1) BS: 88 (70-179) Na: 119 (135-145) K: 4.3 (3.5-5.1) Random urine Na: 93 (20-40) Urine specific gravity: 1023 Acid uric: 3.7 (2.5-5.5) ESR: 16 (< 14) CRP: 3.2 (up to 6) B/C: No growth CSF WBC: 210 (PMN: 70% - MN: 30%) CSF Protein: 130 (15-45) CSF Lactate: 16 (10-22) CSF LDH: 518 CSF Glucose: 51 (>2/3 blood sugar) CSF culture: No growth |
Discussion
We were facing a case of cerebrovascular complication of craniopharyngioma surgery, 2 weeks after initial resection with neurological deficits.
However, there is no clear reason to explain delayed vasospasm; and due to the few reports in this field, no protocol for the prevention and management of this issue, following skull base tumor resection; it comes to mind that various causes are involved [1,5].
The presence of subarachnoid blood in the postoperative period, direct surgical injury to the blood vessels in the basal cisterns, Hypothalamic damage, secretion of chemicals or spasmogenic factors, and spillage of fluid from the craniopharyngioma cyst that induces chemical meningitis; is considered as the main causes for delayed vasospasm [6-10].
To the best of our knowledge, there are six previously reported cases of cerebral vasospasm following craniopharyngioma endoscopic resection which is mostly noted in the first 2 weeks [1,11-14]. To date, this case report is the second one that is complicated by severe DI and CSW with rapid fluid and electrolyte shifts. In 2017 Dr. Singh et al. report a series of 6 patients who had craniopharyngioma surgery and progressed to cerebral vasospasm. They revealed that electrolyte and fluid imbalance is caused by different phases of DI and CSW. Besides that, dehydration secondary to severe DI and hypocortisolic state following early steroid tapering leads to the deterioration of the vasospasm [14].
In 2015 a case report in Italy reports volume depletion following DI cause cerebral hypoperfusion and worsening resultant ischemia [13].
Our patient’s course was complicated by acute severe hyponatremia; electrolyte and fluid imbalance caused by Hypothalamic-Pituitary Axis (HPA) impairment may involve in the deterioration of vasospasm [15].
Syndrome of Inappropriate Antidiuretic Hormone secretion (SIADH) and Cerebral Salt-Wasting Syndrome (CSWS) are the most common causes of hyponatremia in patients with neurological problems [16,17].
CSWS and SIADH are not possible to differentiate based on serum and urine laboratory findings alone, because the associated abnormalities are identical [18].
The proper diagnosis of SIADH requires the detection of urine and serum osmolality, urinary sodium, cortisol, and thyroid hormone [19].
Our patient underwent replacement therapy after the primary surgery and at the time of admission, he had adrenal and thyroid axis coverage there was hypovolemia with serum hypo osmolarity, and also increased urine sodium levels with polyuria and low blood pressure, leading to the diagnosis of CSWS. with keeping in mind that prolonged dehydration in CSWS may have caused vasospasm and ischemia in this patient.
Accurate determination of the patient’s volume status is the key to differentiating these syndromes. Unfortunately, the determination of volume status is very difficult to do accurately in routine clinical practice.
However, we believe that cerebral vasospasm following craniopharyngioma resection must be considered in differential diagnosis, and timely diagnosis and treatment improve outcomes beside its rarity makes this situation very challenging [13].
Conclusion
In the setting of acute neurological deterioration after craniopharyngioma resection, the diagnosis of cerebral vasospasm due to electrolyte, and fluid imbalance especially CSW, should be in the differential and early diagnosis and timely treatment will improve the patient’s outcome.
Conflict of interest: There is no conflict of interest.
References
- Salunke P, Sodhi HBS, Aggarwal A, Ahuja CK. Delayed cerebral vasospasm following surgery for craniopharyngioma. Journal of neurosciences in rural practice. 2013; 4(01): 107-9.
- Vergouwen MD, Hemorrhage PitIM-DCCotCCMoS. Vasospasm versus delayed cerebral ischemia as an outcome event in clinical trials and observational studies. Neurocritical care. 2011; 15(2): 308.
- Chong MY, Quak SM, Chong CT. Cerebral ischaemia in pituitary disorders—more common than previously thought: two case reports and literature review. Pituitary. 2014; 17: 171-9.
- Macdonald RL, Hoffman HJ. Subarachnoid hemorrhage and vasospasm following removal of craniopharyngioma. Journal of Clinical Neuroscience. 1997; 4(3): 348-52.
- Molina ES, Di Somma A, Stummer W, Briganti F, Cavallo LM. Clinical vasospasm after an extended endoscopic endonasal approach for recurrent pituitary adenoma: illustrative case and systematic review of the literature. World Neurosurgery. 2019; 128: 29-36.
- Connolly Jr E, Rabinstein A, Carhuapoma J, Derdeyn C, Dion J, Higashida R, et al. American Heart Association Stroke Council; Council on Cardiovascular Radiology and Intervention; Council on Cardiovascular Nursing; Council on Cardiovascular Surgery and Anesthesia; Council on Clinical Cardiology. Guidelines for the management of aneurysmal subarachnoid hemorrhage: a guideline for healthcare professionals from the american heart association/american stroke association. Stroke. 2012; 43(6): 1711-37.
- Nishioka HI, J. Haraoka, H. Cerebral vasospasm following transsphenoidal removal of a pituitary adenoma. British journal of neurosurgery. 2001; 15(1): 44-7.
- Shida N, Nakasato N, Mizoi K, Kanaki M, Yoshimoto T. Symptomatic Vessel Narrowing Caused by Spontaneous Rupture of Craniopharyngioma Cyst—Case Report—. Neurologia medico-chirurgica. 1998; 38(10): 666-8.
- Bejjani GK, Sekhar LN, Yost A-M, Bank WO, Wright DC. Vasospasm after cranial base tumor resection: pathogenesis, diagnosis, and therapy. Surgical neurology. 1999; 52(6): 577-84.
- Ecker RD, Atkinson JL, Nichols DA. Delayed ischemic deficit after resection of a large intracranial dermoid: case report and review of the literature. Neurosurgery. 2003; 52(3): 706-10.
- Nash R, Elwell V, Brew S, Powell M, Grieve J. Management strategy for treatment of vasospasm following transsphenoidal excision of craniopharyngioma. Acta neurochirurgica. 2016; 158: 2105-8.
- Hansen D, Hidalgo J, Cohen A, Mukherjee D, Scafidi S. Evaluation and Management of Symptomatic Vasospasm following Endoscopic Endonasal Resection of Pediatric Adamantinomatous Craniopharyngioma. Case Reports in Pediatrics. 2020.
- Ricarte IF, Funchal BF, Alves MAM, Gomes DL, Valiente RA, Carvalho FA, et al. Symptomatic cerebral vasospasm and delayed cerebral ischemia following transsphenoidal resection of a craniopharyngioma. Journal of Stroke and Cerebrovascular Diseases. 2015; 24(9): e271-e3.
- Singh A, Salunke P, Rangan V, Ahuja CK, Bhadada S. Vasospasm after craniopharyngioma surgery: Can we prevent it? World Neurosurgery. 2017; 101: 208-15.
- Alzhrani G, Sivakumar W, Park MS, Taussky P, Couldwell WT. Delayed complications after transsphenoidal surgery for pituitary adenomas. World Neurosurgery. 2018; 109: 233-41.
- Kalita J, Singh RK, Misra UK. Cerebral salt wasting is the most common cause of hyponatremia in stroke. Journal of Stroke and Cerebrovascular Diseases. 2017; 26(5): 1026-32.
- Moritz ML. Syndrome of inappropriate antidiuresis. Pediatric Clinics. 2019; 66(1): 209-26.
- Yee AH, Burns JD, Wijdicks EF. Cerebral salt wasting: pathophysiology, diagnosis, and treatment. Neurosurgery Clinics. 2010; 21(2): 339-52.
- Spasovski G, Vanholder R, Allolio B, Annane D, Ball S, Bichet D, et al. Clinical practice guideline on diagnosis and treatment of hyponatraemia. Nephrology Dialysis Transplantation. 2014; 29(suppl_2): i1-i39.