
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Research Article - Open Access, Volume 4
A retrospective study of flap selection for through-and-through cheek defect reconstruction
*Corresponding Author : Tian Hao
283 Tongzipo Road, Changsha City, Hunan Province, China.
Email: tianhao01262023@163.com
Received : Jul 10, 2023
Accepted : Aug 21, 2023
Published : Aug 28, 2023
Archived : www.jcimcr.org
Copyright : © Hao T (2023).
Abstract
This retrospective study compared different reconstructive strategies for through-and-through cheek defects arising from radical resection of buccal squamous cell carcinoma. Based on clinical data collected from March 2016 to September 2021, the study included 96 patients with buccal squamous cell carcinoma that underwent radical resections and subsequent reconstructions. The reconstructions involved with three different reconstructive methods: free flaps only, free flaps combined with local flaps, local flaps only. The reconstructive outcomes were compared in terms of postoperative oral function and aesthetics. The results showed that local flaps produced better aesthetics outcomes than ALT free flaps did; stretching vermilion myocutaneous flaps yielded better functional and aesthetic results than suturing freed vermilion myocutaneous flaps with ALT free flaps or local flaps in terms of repairing lips and oral commissure defects. Based on the results, it is concluded that a bi-paddle ALT free flap with a single pedicle is a good option for reconstructing substantial buccal defects. Local flaps are a good fit for reconstructing small-to-medium buccal defects. If the cheek defect involves lips and oral commissure, vermilion myocutaneous flaps should be lifted and stretched to repair lips and oral commissure defects. The 3D printing technology contributes to patient-specific surgical planning and reconstruction. Besides, surgeons must have the idea of oncoplastic surgery and master multiple reconstructive methods and procedures.Ultimately, better functional and aesthetic results can be achieved and patient quality of life will be improved.
Keywords: Through-and-through cheek defect; ALT free flaps; Local flaps; Vermilion myocutaneous flaps; 3D printing technology; Patient-specific reconstruction.
Citation: Hao T. A retrospective study of flap selection for through-and-through cheek defect reconstruction. J Clin Images Med Case Rep. 2023; 4(8): 2563.
Introduction
Squamous Cell Carcinoma (SCC) of the buccal mucosa is a common and widespread oral and maxillofacial cancer in Central and Southeast Asia [1,3,4]. Buccal mucosa SCC is a locoregionally aggressive tumor that develops and spreads fast, because no fixed anatomic barrier exists to prevent it from growing and invading neighboring areas, such as mandible, maxilla, lips, and cheek skin [3-6]. The invasion to surrounding areas often demands a radical excision that creates through-and-through cheek defects. Reconstructing through-and through cheek defects has always been a challenge for surgeons, because of the defect’s conspicuous site, limited local tissue supply, and vicinity to several structures of important function [7]. In addition, a successful full-thickness cheek reconstruction is highly demanding. It requires three-dimensional restoration of all missing components and simultaneous repairment of both intraoral mucosa and extraoral skin [8,9]. A successful reconstruction not only restores the function, but also improves postoperative appearance. The key to a successful reconstruction is the appropriate choice of flap, which is mainly based on the surgeons’ experience and preference and often corresponds to none systematic indication [8,10].
For centuries, local flaps were dominant in defect reconstructions [11]. Since 1970s, with the development of vascular anastomosis and microsurgery, free flaps have become the first option for reconstructing oncological defects in oral and maxillofacial region [11,12]. However, neither local flaps nor free flaps are perfect. Local flaps provide good color and texture match due to their proximity to the defect and lead to good aesthetic outcomes, but they do not have adequate soft tissue for reconstructing extensive composite defects [13-15]. By contrast, free flaps have enough volume of bone, skin, and muscle and thus are versatile for repairing sizable defects, but they usually achieve inferior aesthetic outcomes than local flaps do [16]. Therefore, a combination of local flaps and free flaps might achieve a more ideal reconstructive result [17].
The intent of our study is to provide surgeons with the flap selection tailored to specific characteristics of defects in full-thickness cheek reconstruction. Since 2004, our department has been using varied local and free flaps to reconstruct oncological defects in oral and maxillofacial region, with a significant number of them being through-and-through cheek defects resulting from buccal SCC resections. Based on our clinical experience, we compared the reconstructive techniques and outcomes for repairing through-and-through cheek defects and summarized our understanding of choice of flaps. We also explored the role of 3D printing technology in surgical planning and reconstructive strategy.
Materials and methods
Patient demographics
From March 2016 to September 2021, 96 patients who underwent radical resections and reconstructions were included in the study. The inclusion criteria were: (1) the patient was histologically confirmed with primary buccal SCC; (2) the patient did not receive surgery, chemotherapy, radiotherapy, or any other treatment before radical surgery; (3) the patient had a through-and-through cheek defect as a result of radical surgery. Patients who had distant metastasis were excluded. All patients signed the informed consent form.
Primary tumor resection and reconstruction
The primary tumor resection was radical resection that referred to the Unit Resection Buccal Surgery (URBS) [8]. After resection, the resultant bony defects, through-and-though cheek defects, and/or lips and oral commissure defects were immediately reconstructed with flaps. Only one mandible bony defect underwent bony reconstruction with a fibular free flap (FibF) and all the other maxillary and mandible bony defects underwent soft-tissue reconstructions only. It’s because soft-tissue reconstruction takes less time to heal and patients can receive adjuvant therapies on time. Soft-tissue reconstructions involved one of the three methods: free flaps only, free flaps combined with local flaps, and local flaps only. The reconstructive methods used in the study are summarized in table 2.
Of 96 patients, 48 patients had through-and-through cheek defects involving lips and oral commissure. Lips and oral commissure defects were reconstructed with vermillion myocutaneous flaps by two different approaches: stretch the raised vermillion myocutaneous flaps or suture the free ends of flaps to the raised vermilion myocutaneous flaps to bridge the loss. Table 3 summarizes reconstructive methods for lips and oral commissure defects.
Evaluation of reconstructive outcomes
All 96 patients after discharge underwent regular follow-up evaluations that lasted at least 6 months. The follow-up evaluations were recorded at the surgeon’s outpatient clinic and the cancer case management center of the hospital. During the follow-up period, patients were tested and recorded for their postoperative oral functions and aesthetic results. The oral function assessment consisted of mouth opening and orbicularis oris muscle’s function. The mouth opening was rated as normal = 4.5 cm, I = 3 cm, II = 1.5 cm, III = narrower than the width of the patient’s index finger, and IV = cannot open the mouth. The orbicularis oris muscle’s function was rated as 1 = unable to suck water with a straw, 2 = can suck some water with a straw, and 3 = can suck water with a straw [18,19]. The aesthetic result was rated as: 1- unsatisfactory, 2- satisfactory, and 3-excellent [18].
Results
Survival rate of flaps and postoperative complications
93 (96.9%) patients had primary healing, and 3 (3.1%) patients encountered healing problems [1]. Patient reconstructed with a bi-paddle ALT free flap had total flap necrosis and underwent a salvage surgery; 1 patient reconstructed with a single-paddle ALT free flap had a venous crisis and underwent emergency surgery. After the paddle was trimmed and the tension on the pedicle and the paddle was reduced, the flap survived; 1 patient reconstructed with local flaps had intraoral partial flap necrosis and were recovered after debridement and dressing change.
Postoperative mouth opening and the function of orbicularis oris muscle
In terms of postoperative mouth opening, for 20 patients whose lip defects were smaller than 1/3 of the width of the vermilions, 3 were grade I, 16 were grade II, and 1 were grade III; for 16 patients whose lip defects were between 1/3 and 1/2 of the width of the vermilions, 6 had normal mouth opening, 5 were grade II, and 5 were grade III; for 12 patients whose lip defects were larger than 1/2 of the width of the vermilions, all had normal mouth opening. Of the 48 patients without lips defects, 29 had normal mouth opening, 13 were grade I, and 6 were grade II. They had either grade 2 or 3 postoperative orbicularis oris muscle’s function.
Postoperative aesthetic results
Regardless of lips and oral commissure defects, patients reconstructed with local flaps had the best aesthetic results. Patients reconstructed with bi-paddle ALT free flaps had better aesthetic results than those reconstructed with single-paddle ALT free flaps.

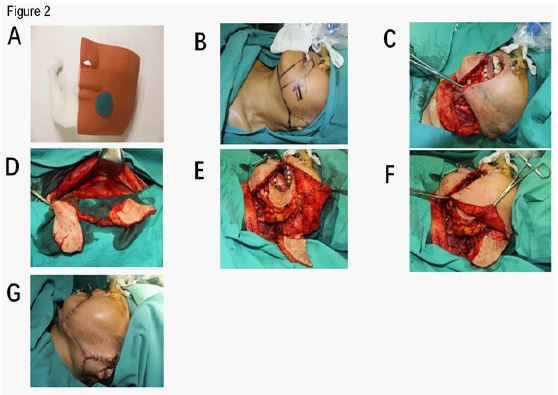

Table 1: Characteristics of patients in the study (n=96).
| Characteristics | Value (%) | % |
|---|---|---|
| Age | 58.4 (33-70) | |
| Sex | ||
| Male | 70 | 72.9 |
| Female | 26 | 27.1 |
| T staging | ||
| T2 | 4 | 4.2 |
| T3 | 23 | 24.0 |
| T4 | 69 | 71.8 |
| Differentiation | ||
| Well differentiated | 63 | 65.6 |
| Moderately differentiated | 27 | 28.1 |
| Poorly differentiated | 6 | 6.3 |
Table 2: Summary of reconstructive methods.
| Free flaps only | Free flaps combined with local flaps | Local flaps only | % | |
|---|---|---|---|---|
| ALT free flap (bi-paddle) | 13 | - | - | free flaps only: 22.9 |
| ALT free flap (single-paddle) | 8 | - | - | |
| ALT free flap (bi-paddle) + FibF | 1 | - | - | |
| ALT free flap (bi-paddle) + advancement flap | - | 10 | - | free flaps combined with local flaps: 49.0 |
| ALT free flap (single-paddle) + advancement flap | - | 5 | - | |
| vermilion myocutaneous flap + ALT free flap (bi-paddle or single-paddle) | - | 32 | - | |
| vermilion myocutaneous flap + advancement flap | - | - | 16 | local flaps only: 28.1 |
| SAIF + advancement flap | - | - | 6 | |
| SAIF + advancement flap + rotation flap | - | - | 5 | |
| Total | 22 | 47 | 27 | 96 |
FibF: Fibular free flap; SAIF: the supraclavicular artery island flap.
Table 3: Reconstructive methods for lips and oral commissure defects, and corresponding postoperative functional and esthetic results.
| Reconstructive Methods Variables |
< 1/3 of the vermilion | 1/3-1/2 of the vermilion | >1/2 of the vermilion | |
|---|---|---|---|---|
| Stretch the freed vermilion myocutaneous flaps | Stretch the freed vermilion myocutaneous flaps | Suture ALT free flaps or local flaps to the freed vermilion myocutaneous flaps | Suture ALT free flaps or local flaps to the freed vermilion myocutaneous flaps | |
| Functional results | ||||
| Maximum mouth opening | ||||
| Normal | 0 | 0 | 6 | 12 |
| I | 3 | 0 | 0 | 0 |
| II | 16 | 5 | 0 | 0 |
| III | 1 | 5 | 0 | 0 |
| Orbicularis oris muscle’s function | ||||
| 1 | 0 | 0 | 4 | 12 |
| 2 | 0 | 4 | 2 | 0 |
| 3 | 20 | 6 | 0 | 0 |
| Aesthetic results | ||||
| 1 | 0 | 0 | 2 | 4 |
| 2 | 4 | 3 | 5 | 8 |
| 3 | 16 | 7 | 0 | 0 |
Table 4: postoperative functional and esthetic results of cheek reconstructions without lips and oral commissure defects.
| Variables | ALT(bi–paddle) | ALT (single-paddle) | Local flaps only |
|---|---|---|---|
| Aesthetic results | |||
| 1 | 0 | 0 | 0 |
| 2 | 6 | 6 | 3 |
| 3 | 18 | 7 | 8 |
Discussion
Surgical resection remains the standard treatment for resectable oral and maxillofacial cancers [20]. In oral and maxillofacial cancer surgery, radical resection usually removes the primary tumor along with its 1.5 cm circumferential margin [4,21]. The incisal margins were then sent for the intraoperative frozen pathological examination to determine final resection area [22]. The resection area usually involves partial or total adjacent structures, producing defects of varying sizes and contours [23]. These defects are unfit for direct closure because direct closure impairs oral function and worsens appearance, especially through-and-through cheek defects. Through-and-through cheek defects require immediate flap reconstructions, which has always been a challenge for surgeons.
We concluded that a bi-paddle ALT free flap with a single pedicle is a better option than a folded single-paddle ALT free flap for reconstructing extensive and complex oral and maxillofacial defect. As shown in the results, patients reconstructed with a bi-paddle ALT free flap have better aesthetic results. The reasons are as follow: the pliable skin paddles can be more flexibly positioned at the defect and can be more easily trimmed and de-epithelialized to a proper size, shape, and thickness, both of which make they fit the defect better and yields better aesthetic outcomes. Besides, the two paddles have a better blood circulation, which guarantees a higher survival rate. The most distinctive attribute of the bi-paddle ALT free flap with a single pedicle is its capability to repair both intraoral mucosa lining and extraoral skin lining at the same time [24]. However, harvesting a bi-paddle ALT free flap with a single pedicle is more difficult and time-consuming. Two perforators that have a proper distance in between and proper calibers are occasionally absent in the donor site. Those who lack such two perforators are not available for reconstruction with a bi-paddle ALT free flap, and the alternative is a folded single-paddle ALT free flap. A clinical scenario in our study where a bi-paddle ALT free flap is also preferred for reconstruction is advanced buccal SCC with extensive mandible bone infiltration, especially the infiltration of mandibular ramus.
To reconstruct less sizable defects with widths smaller than 4 cm, local flaps should be used for improved aesthetic outcomes. It’s due to local flaps’ ability to reconstruct defects with “like” tissue [25]. After buccal SCC resection, the size of extraoral skin defect is usually smaller than that of intraoral mucosa defect. Consequently, local flaps can be used to repair the extraoral skin defect while ALT free flaps or supraclavicular artery island flap (SAIF) can be used to repair intraoral defect. According to the results, local flap reconstruction involving advancement flaps or SAIF, achieves satisfactory aesthetic outcomes. As figure 2 shows, the advancement flap extended to cover the skin defect in the frontal facial area, moving the skin defect to a less visible site near the ear. Then a bi-paddle ALT free flap was used to repair the intraoral defect and the well-placed skin defect, one paddle for each. The reconstruction resulted in a well-camouflaged scar line and improved postoperative esthetics. However, the design and harvest of local flaps should follow the rules: (1) the width of the local flap lifted should be larger than that of intraoral defect; (2) the local flap’s length-to-width ratio must be appropriate. Appropriate length-to-width ratio ensures the direct closure of the donor site [13]. As shown in figure 3, besides advancement flap, SAIF can be used to repair limited-sized oral cavity defects involving mandible. SAIF belongs to local perforator flaps, which represent a promising new area in reconstructive surgery and offer several brand-new flap options [26,27]. For elderly patients with increased skin laxity, the local flap can be raised larger and wider, because increased skin laxity with aging often allows for substantial tissue mobilization, transfer, and advancement [7]. Other flaps that are good alternatives and achieve satisfactory functional and aesthetic results include folded pectoralis major muscle flap (PMMF), folded extended supraclavicular fasciocutaneous island flap (SFIF), folded extended vertical lower trapezius island myocutaneous flap (TIMF), and Abbe–Estlander flap (A-EF) [13,19,26,28-30].
The anterior buccal SCC usually infiltrates along the orbicularis oris muscle and crosses the oral commissure to reach vermilions, necessitating radical resection of the affected portion of oral commissure and vermilions [33]. The one-stage reconstruction of the remaining oral commissure and vermilions is challenging because their morphology is hard to restore [8,19,25]. The restoration involves the vermilion myocutaneous flap to cover intraoral and extraoral defects, maintains sufficient oral competence and oral access, and recovers vermilion configuration and appearance [15,25,34]. In our study, vermilion myocututaneous flaps were used to resurface lips and oral commissure defects. Based on the results, we concluded that when the defect is smaller than 1/3 of the width of the vermilions, vermilion myocututaneous flaps should be freed and stretched to close the lips and oral commissure defect. As shown in the results, all 20 patients had good postoperative oral competence. Although most patients didn’t recover normal mouth openings, all of them had acceptable mouth opening degrees and none of them had drooling. Most patients had occasional or continuous drooling, which severely lowers their quality of life and should be avoided. When the defect is between 1/3 and 1/2 of the width of the vermilions, the priority of lips and oral commissure reconstruction is to avoid postoperative drooling in patients. Second comes the mouth opening. The mouth opening should suffice normal speech and food ingestion. If necessary, a second-stage reconstruction could be carried out to enlarge the mouth opening. In conclusion, stretching the freed vermilion myocututaneous flaps to close lips and oral commissure defect is recommended because it gives a good overall reconstructive outcome.
Conclusion
In conclusion, reconstructing through-and-through cheek defects arising from tumor resection is a challenge. Since standard instrumentation for flap selection doesn’t exist, animated discussions among surgeons regrading what is the “ideal flap” for repairing a certain defect never stops [27]. However, when choosing the suitable flap, surgeons should take patient characteristics, such as age, skin laxity, needs for adjuvant modalities and defect characteristics, such as size, depth, and shape into consideration. Our study provides surgeons with customized flap options for reconstructing full-thickness cheek defects. The right choice of flap is the cornerstone of a successful reconstruction. The design of surgical incisions for extraoral skin should follow aesthetic subunit principle and surgeons should pay attention to suturing techniques to reduce surgical scars [8,27,35]. In addition, the 3D-printed model should be used for customized reconstructive design. However, so far 3D printing technology has not yet become one of the standard workups for surgical patients, but it has the potential to become an indispensable part of clinical practice in the future. Ultimately, a patient-specific flap selection and a meticulous reconstruction will benefit patients and achieve long-term functional and aesthetic success.
References
- Chen J, He QY, Yuen APW, Chiu JF. Proteomics of buccal squamous cell carcinoma: The involvement of multiple pathways in tumorigenesis. Proteomics. 2004; 4(8): 2465-2475. doi:10.1002/pmic.200300762
- Zhou X, Wang W. Oncoplastic Surgery. 2018. doi:10.22551/2018.20.0503.10130
- Deconde A, Miller ME, Palla B, et al. Squamous cell carcinoma of buccal mucosa: A 40-year review. Am J Otolaryngol - Head Neck Med Surg. 2012; 33(6): 673-677. doi:10.1016/j.amjoto.2012.04.006
- Ren Z, Gong Z, Wu H. Unit resection of buccal squamous cell carcinoma : Description of a new surgical technique. 2017; 8(32): 52420-52431.
- Strome SE, To W, Strawderman M, et al. Squamous cell carcinoma of the buccal mucosa. Otolaryngol - Head Neck Surg. 1999; 120(3): 375-379. doi:10.1016/S0194-5998(99)70278-0
- Marinelli LM, Chatzopoulos K, Marinelli JP, et al. Clinicopathologic predictors of survival in buccal squamous cell carcinoma. J Oral Pathol Med. 2020; 49(9): 857-864. doi:10.1111/jop.13046
- Heller L, Cole P, Kaufman Y. Cheek Reconstruction: Current Concepts in Managing Facial Soft Tissue Loss. Semin Plast Surg. 2008; 22(04): 294-305. doi:10.1055/s-0028-1095888
- Gong ZJ, Ren ZH, Wang K, Tan HY, Zhang S, Wu HJ. Reconstruction design before tumour resection: A new concept of through-and-through cheek defect reconstruction. Oral Oncol. 2017; 74(139): 123-129. doi:10.1016/j.oraloncology.2017.09.023
- Bucci T, Fior A, Nocini PF. Reconstruction of full-thickness cheek defect with a folded cervico-pectoral cutaneous flap following ablation of advanced oral cancer in elderly patient. Eur J Plast Surg. 2018; 41(1): 89-92. doi:10.1007/s00238-017-1350-7
- Chang JW, Lim JH, Lee JH. Reconstruction of midface defects using local flaps. Medicine (Baltimore). 2019; 98(46): e18021. doi:10.1097/md.0000000000018021
- Steel BJ, Cope MR. A brief history of vascularized free flaps in the oral and maxillofacial region. J Oral Maxillofac Surg. 2015; 73(4): 786.e1-786.e11. doi:10.1016/j.joms.2014.12.005
- Bouguila J. Through and through cheek defects: a systematic review and proposition of a classification. Int J Oral Maxillofac Surg. 2017; 46: 10-11. doi:10.1016/J.IJOM.2017.02.038
- Goh CSL, Perrett JG, Wong M, Tan BK. Delayed bipedicled nasolabial flap in facial reconstruction. Arch Plast Surg. 2018; 45(3): 253-258. doi:10.5999/aps.2017.00878
- Yang SF, Truesdale C, Moyer JS. LOCAL FLAPS FOR FACIAL RECONSTRUCTION. Open Access Atlas Otolaryngol Head Neck Oper Surg. 2016;Volume 1-. doi:10.15641/0-7992-2534-1
- Wen-Chung Liu K-CY. One-stage through-and-through cheek, lips, and oral commissure reconstruction using a double-paddle peroneal chimeric flap: An innovative method. Head Neck. 2014; 36(10): 1391. doi:10.1002/Hed.23658
- Gabrysz-Forget F, Tabet P, Rahal A, Bissada E, Christopoulos A, Ayad T. Free versus pedicled flaps for reconstruction of head and neck cancer defects: A systematic review. J Otolaryngol - Head Neck Surg. 2019; 48(1): 1-31. doi:10.1186/s40463-019-0334-y
- Futran ND, Mendez E. Developments in reconstruction of midface and maxilla. Lancet Oncol. 2006; 7(3): 249-258. doi:10.1016/S1470-2045(06)70616-7
- de Caxias FP, dos Santos DM, Goiato MC, et al. Effects of mouth rehabilitation with removable complete dentures on stimulus perception and the electromyographic activity of the orbicularis oris muscle. J Prosthet Dent. 2018; 119(5): 749-754. doi:10.1016/j.prosdent.2017.07.017
- Chen WL, Wang Y, Zhou B, Liao JK, Chen R. Comparison of the reconstruction of through-and-through cheek defects involving the labial commissure following tumor resection using four types of local and pedicle flaps. Head Face Med. 2019; 15(1): 1-9. doi:10.1186/s13005-019-0196-6
- Sakamoto Y, Yanamoto S, Ota Y, Furudoi S, Komori T, Umeda M. Magnitude of Myocutaneous Flaps and Factors Associated with Loss of Volume in Oral Cancer Reconstructive Surgery. J Oral Maxillofac Surg. 2016; 74(3): 644-649. doi:10.1016/j.joms.2015.09.021
- De Virgilio A, Iocca O, Di Maio P, et al. Head and neck soft tissue reconstruction with anterolateral thigh flaps with various components: Development of an algorithm for flap selection in different clinical scenarios. Microsurgery. 2019; 39(7): 590-597. doi:10.1002/micr.30495
- Cai YC, Li C, Zeng DF, et al. Comparative analysis of radial forearm free flap and anterolateral thigh flap in tongue reconstruction after radical resection of tongue cancer. Orl. 2019; 81(5-6): 252-264. doi:10.1159/000502151
- Mittal G, Agarwal A, Kataria G. Flaps for Oral and Maxillofacial Reconstruction : Review of Literature and a Clinical Guide to the Clinicians. Published online 2018.
- Park CW, Miles BA. The expanding role of the anterolateral thigh free flap in head and neck reconstruction. Curr Opin Otolaryngol Head Neck Surg. 2011; 19(4): 263-268. doi:10.1097/MOO.0b013e328347f845
- Fata JJ. The vermilion myomucosal flap for the treatment of oral commissure gunshot wound deformities. Plast Reconstr Surg. 1999;103(1):197-201. doi:10.1097/00006534-199901000-00032
- Razdan SN, Albornoz CR, Ro T, et al. Safety of the Supraclavicular Artery Island Flap (SAIF) in the setting of neck dissection and radiation therapy. 2015; 31(5): 378-383. doi:10.1055/s-0035-1546294.Safety
- Maciel-Miranda A, Morris SF, Hallock GG. Local flaps, including pedicled perforator flaps: Anatomy, technique, and applications. Plast Reconstr Surg. 2013; 131(6): 896-911. doi:10.1097/PRS.0b013e31828bd89f
- Alvarez GS, Siqueira EJ, De Oliveira MP. A new technique for reconstruction of lower-lip and labial commissure defects: A proposal for the association of Abbe-Estlander and vermilion myomucosal flap techniques. Oral Surg Oral Med Oral Pathol Oral Radiol. 2013; 115(6): 724-730. doi:10.1016/j.oooo.2012.10.009
- Rifaat MA. Reconstruction of medium-sized defects of oral commissure by combining double full-thickness cheek rhomboidal flaps and a small lip switch flap. Ann Plast Surg. 2011; 67(2): 134-138. doi:10.1097/SAP.0b013e3181f3e315
- Sakakibara A, Matsumoto K, Hasegawa T, Minamikawa T, Komori T. Single-stage reconstruction for buccal mucosa tumor resection including the labial commissure using a facial artery musculomucosal flap and a vermilion advancement flap. J Surg Case Reports. 2017; 2017(6): 1-4. doi:10.1093/jscr/rjx108
- Burusapat C, Pitiseree A. Advanced squamous cell carcinoma involving both upper and lower lips and oral commissure with simultaneous reconstruction by local flap: A case report. J Med Case Rep. 2012; 6(1): 23. doi:10.1186/1752-1947-6-23
- Goldstein MH. A tissue-expanding vermilion myocutaneous flap for lip repair. Plast Reconstr Surg. 1984; 73(5): 768-770. doi:10.1097/00006534-198405000-00008
- Gauglitz GG. Textbook on Scar Management.; 2020. doi:10.1007/978-3-030-44766-3