
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Cognitive-linguistic diagnostic profile of anomic aphasia in moyamoya disease: A case study
*Corresponding Author : Sandhya K
Assistant Professor, Speech Language Pathology, SDM College of Medical Sciences and Hospital, SDM University, Dharwad, India.
Tel: 9035362883;
Email: sandhyak@sdmmedicalcollege.org
Received : Aug 01, 2023
Accepted : Aug 21, 2023
Published : Aug 28, 2023
Archived : www.jcimcr.org
Copyright : © Sandhya K (2023).
Abstract
Moyamoya syndrome is a type of progressive cerebro vascular disorder characterised by progressive narrowing of arteries of the circle of Willis. Arteries get clogged because of growth of prominent small vessel due to which blood supply to the brain is reduced [1]. A 31 years old male was a pre-diagnosed case of Moyamoya Disorder (MMD) with hemiplegia of right side. His MRI reports revealed Magnetic Resonance Imaging brain angiogram was done which showed patchy left Middle Cerebral Artery (MCA) territory infarcts with involvement of left anterior basal ganglia, left insular cortex and patchy frontal and parietal infarcts as well as left Internal Carotid Artery (ICA) occlusion. He presented with a complaint of difficulty in recalling names. Based on Medical history, formal and informal evaluations, the patient was diagnosed as having Anomic Aphasia with Cognitive deficit secondary to MMD. The case study has attempted to provide a comprehensive picture of the patient’s cognitive linguistic profile.
Keywords: Moyamoya disorder; MMD; Anomic aphasia; Cognitive-linguistic disorder.
Citation: Sandhya K. Cognitive-linguistic diagnostic profile of anomic aphasia in moyamoya disease: A case study. J Clin Images Med Case Rep. 2023; 4(8): 2564.
Introduction
Moyamoya syndrome is a type of progressive cerebro vascular disorder characterised by progressive narrowing of arteries of the circle of Willis. Arteries get clogged because of growth of prominent small vessel. As a result, blood supply to the brain is reduced [1]. Despite the fact that it can be found all over the world, it is more widespread in East Asian countries. Two peaks of onset are observed in Moyamoya syndrome where one is in childhood and the other is in young adulthood [2]. The ischemic type has been shown to be predominate in childhood, while the hemorrhagic type is more often observed in the adult population [3].
This disorder is characterised by hazy appearance on angiography resembling a puff of smoke in the air and has thus been given the name Moyamoya, a Japanese term meaning the same. Japan has the highest incidence of MMD, with three cases per 100,000 [1]. The clinical presentation of MMD includes Transient Ischemic Attacks (TIA), ischemic stroke, hemorrhagic stroke, headache, epilepsy and cognitive dysfunction [4]. Clinical profile of MMD includes headache, cognitive impairment, hypertension, temporary or permanent blindness, hemiplegia, general paresis of the insane, loss of sensation, aphasia, and mechanisms related to ischemia in the frontal, parietal, and temporal lobes [5].
Researches have evidenced that Moyamoya disease is associated with Cognitive deficits and aphasia. An estimated one million individuals in the United States have aphasia and an estimated 80,000 new cases are thought to be diagnosed each year (American Speech-Language-Hearing Association [ASHA], 2014b) [6]. Aphasia is an acquired condition caused by a disease or trauma to parts of the brain involved in language processing. According to ASHA (2014b) [6], the most prevalent cause of aphasia is stroke. An estimated 25-40% of stroke survivors are diagnosed with aphasia (National Aphasia Association, 2014) [7]. It may affect auditory comprehension, verbal expression, reading, and writing and word-finding abilities along with sensory-motor impairments. Anomic aphasia can be a difficulty in retrieving precise nouns, often intended words, but occasionally verbs, when creating sentences. Although the grammatical features of the sentence remain intact, word retrieval difficulty persists that leads to insertion of filler words, long pauses or choice of wrong words (paraphasias) [8]. Though there are a couple of case reports on cognitive deficits in adults with MMD, limited Indian researches available which documents the structured assessment of language and cognitive abilities and hence, the present study gives a picture of detailed evaluation of a patient of MMD.
Case presentation
A 31 years old male, presented with sudden onset of right side weakness and inability to speak since that morning. The patient is married and works as a Software Engineer. The patient reported to the department of Speech and Hearing with a complaint of difficulty in recalling names. He was a prediagnosed case of MMD with hemiplegia of the right side.
Medical history
On arrival, his Blood Pressure (BP) was 150/100 mmgh, Glassgow Coma Scale (GCS) E4M5V1, pupils 2 mm. He complained of slurring of speech and inconsistent response to name call. Magnetic Resonance Imaging brain angiogram was done which showed patchy left Middle Cerebral Artery (MCA) territory infarcts with involvement of left anterior basal ganglia, left insular cortex and patchy frontal and parietal infarcts as well as left Internal Carotid Artery (ICA) occlusion. The patient was intubated and admitted for Digital Subtraction Angiography (DSA) and emergency mechanical thrombectomy. DSA showed severe narrowing of Left supraclinoid ICA, right terminal ICA and right MCA severe narrowing, left MCA occlusion - likely Moyamoya syndrome.
Mechanical thrombectomy was abandoned in view of DSA finding, Neurosurgery opinion was obtained and patient was admitted in Medical Intensive Care Unit (MICU) started on anti-edema, anticonvulsant, antiplatelets and other neuroprotective measures. Gradually his GCS was improved to E4M6 (to visual cues). CT brain showed Acute- to –subacute infarct in left fronto-temporal operculum, insular cortex, external capsule, caudate and lentiform nuclei. Mass effect with compression of left lateral and 3rd ventricle and midline shift of 5 mm to right, chronic lacunar infarct in right hemisphere and bilateral ethmoid and sphenoid sinusitis was noted. It also showed no significant interval change in infarcts volume and mild effacement of left frontal sulci and gyri.
Language evaluation
On perceptual evaluation, it was noted that he was able to follow commands and give relevant answers to the questions asked. His working memory was intact whereas semantic memory, processing speed and his reasoning were impaired. Speech mechanism examination revealed normal structure and function of articulators. Additionally, he exhibited impaired performance in verbal and visual working memory tasks, while his episodic memory was normal. WAB -K (Kannada version) was administered and AQ of 88.6 was obtained. He performed well in all other domains except Naming.
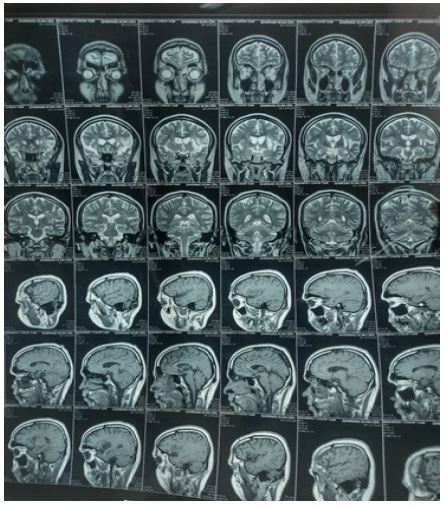
Table 1: WAB scores of the patient.
| WAB domains | Max score | Patient score | AQ |
|---|---|---|---|
| Spontaneous Speech | |||
| Information Content | 10 | 8 | |
| Fluency | 10 | 10 | 18 |
| Comprehension | |||
| Yes/No question | 60 | 60 | |
| Auditory word recognition | 60 | 60 | 9.7 |
| Sequential commands | 80 | 74 | |
| Repetition | |||
| Naming | |||
| Objective Naming | 60 | 56 | |
| Word fluency | 20 | 4 | |
| Sentence completion | 10 | 6 | 7.4 |
| Responsive speech | 10 | 8 | |
| Aphasia quotient | 88.6 |
It was observed that in general conversation he had difficulty in word retrieval. Analysis of speech sample revealed semantic paraphasias (Substitution of another word of same category) and circumlocutions (a deliberate attempt to express a particular word), hesitations and word finding pauses. Naming domain of WAB-K showed impaired word fluency and sentence completion abilities whereas confrontation naming and responsive speech were relatively spared. Based on observation and test results a diagnosis of Anomic Aphasia was made at the Department of Speech and Hearing OPD.
Linguistic Assessment Protocol developed by Aruna (2001) [9] was administered to assess his Cognitive abilities. The CLAP consists of four domains including attention (visual & auditory category), memory (episodic, working & semantic), problem solving (sentence disambiguation, sentence formulation, comparing and contrasting two objects, predicting the outcome of a described situation, Predicting cause of a described situation, answering ‘why’ questions & sequential task analysis) and organization (categorization, analogies & sequencing of events).
With regard to the patient’s cognitive profile, the above mentioned scores show a greater difficulty in attention, perception, discrimination, memory, reasoning and problem solving and organization. Based on all these observations, the patient was diagnosed as having Anomia Aphasia with Cognitive deficit secondary to Moyamoya Syndrome and was subjected to Speech and language therapy.
Table 2: Scores of CLAP of the patient.
| Domain | Test item | Maximum | Patient’s score |
|---|---|---|---|
| I. Attention, Perception and Discrimination | |||
| Visual | Letter Cancellation | 10 | 5 |
| Contingent Letter Cancellation | 10 | 4 | |
| Word Cancellation | 10 | 6 | |
| Auditory | Sound count Letter-Pair | 10 | 2 |
| discrimination Months | 5 | 3 | |
| discrimination Word –Pair | 5 | 2 | |
| backwards naming | 10 | 2 | |
| II. Memory | |||
| Episodic Memory | Orientation and recent memory questions | 10 | 8 |
| Working Memory | Digit Forward | 5 | 5 |
| Digit backward | 5 | 4 | |
| Semantic Memory | Co-ordinate naming | 5 | 3 |
| Super ordinate naming | 5 | 3 | |
| Word-naming fluency | 5 | 2 | |
| Generative naming | 5 | 2 | |
| Sentence repetition | 10 | 6 | |
| Carry out commands | 10 | 5 | |
| III. Reasoning &Problem Solving | |||
| Sentence disambiguation | 10 | 6 | |
| Sentence formulation | 5 | 3 | |
| Predicting outcome | 10 | 5 | |
| Compare and contrast | 10 | 5 | |
| Predicting cause | 10 | 6 | |
| Why Questions | 5 | 2 | |
| Sequential Analysis | 10 | 6 | |
| IV. Organization | Categorization | 10 | 6 |
| Analogies | 10 | 5 | |
| Sequencing events | 40 | 25 | |
Source: Cognitive-linguistic Assessment Protocol for adults (Aruna, 2001) [9].
Discussion
The current study gives a complete Cognitive linguistic profile of a patient of Anomic Aphasia with Cognitive deficits following an MMD induced stroke. The patients with MMD have an increased risk of stroke development, which may be aggravated by pain or anxiety. It is necessary to avoid cerebral ischemic attacks caused by fluctuating BP and respiration. Pre-surgical neuropsychological testing results for persons with MMD reveal that they showed executive functioning impairment with a reasonably unimpaired memory function [10], whereas the current study contradicts the previous evidences. However, several studies have shown significant relationships between language comprehension, for example, and different facets of cognitive control, such as working memory [11] and inhibition [12-14]. A research [11] has shown that performance on a modified listening span task was linked to language comprehension abilities, although only in people with nonfluent aphasia, and not for people with fluent aphasia. Findings of the present investigations appear to be in agreement with previous researches.
Clinical significance
Prior to developing the treatment plan, it is essential to conduct a complete assessment of all relevant criteria, including the degree of involvement and medical history. Additionally, neuropsychological assessments help in formulating intervention plans for maintaining current cognitive performance. Such procedures are essential in continuous rehabilitation efforts and enhance the quality of life for person with Cognitive linguistic disorders. The external validity of the current study, which focuses on a single case profile, is constrained when applied to other MMD cases, but the author expects that this proof will add to the information already available.
References
- Suzuki J, Takaku A. Cerebrovascular “Moyamoya; disease: Disease showing abnormal net-like vessels in base of brain. Arch. Neurol. 1969; 20: 288-299.
- Kuriyama S, Kusaka Y, Fujimura M, Wakai K, Tamakoshi A, et al. Prevalence and Clinicoepidemiological features of Moyamoya disease in Japan. Stroke. 2008; 39: 42-47.
- Burke GM, Burke AM, Sherma AK, Hurley MC, Batjer HH, et al. Moyamoya disease: A summary. Neurosurgical Focus. 2009; 26: E11.
- Zhang H, Zheng L, Feng L. Epidemiology, diagnosis and treatment of moyamoya disease. Exp Ther Med. 2019; 17: 1977-1984.
- Maki Y, Enomoto T. Moyamoya disease. Child’s Nervous System. 1988; 4: 204-212.
- American Speech-Language-Hearing Association [ASHA]. 2014b.
- National Aphasia Association. 2014.
- Sandhya K. Effectiveness of speech and language therapy and spontaneous recovery in anomic aphasia. Journal of Cerebrovascular Sciences. 2020; 8: 101.
- Aruna K. Cognitive linguistic assessment protocol for adults. Unpublished masters dissertation, University of Mysore: Mysore. 2001.
- Karzmark P, Zeifert PD, Tan S, Dorfman LJ. Effect of moyamoya disease on neuropsychological functioning in adults. Neurosurgery. 2008; 62: 1048-51.
- Ivanova MV, Kuptsova SV, Dronkers NF. A comparison of two working memory tasks in aphasia. Aphasiology. 2017; 31: 265-281.
- Kuzmina E, Weekes B. Inhibition and language processing deficits in different types of aphasia. Event abstract. 54th Annual Academy of Aphasia Meeting Conference, Llandudno, Wales, UK. 2016; 10: 16-18.
- Chengappa SK, Kumar R. Normative and clinical data on the Kannada version of Western aphasia battery (WAB-K). Lang India. 2008; 8: 1.
- Glasgow Coma Scale (GCS). Rapid Neurology and Neurosurgery. 2018; 164-165.