
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Short Report - Open Access, Volume 4
Osteitis fibrosa cystica in primary hyperparathyroidism
Suhas Sondur*; Aditya Prasad Panda
Department of Orthopaedics, Kalinga Institute of Medical Sciences, KIIT University, Bhubaneshwar, Odisha, India.
*Corresponding Author : Suhas Sondur
Department of Orthopaedics, Kalinga Institute of Medical Sciences, KIIT University, Bhubaneshwar, Odisha, India.
Tel: +91-7259959943;
Email: sondur.suhas@gmail.com
Received : Aug 05, 2023
Accepted : Aug 24, 2023
Published : Aug 31, 2023
Archived : www.jcimcr.org
Copyright : © Sondur S (2023).
Citation: Sondur S, Panda AP. Osteitis fibrosa cystica in primary hyperparathyroidism. J Clin Images Med Case Rep. 2023; 4(8): 2570.
Image description
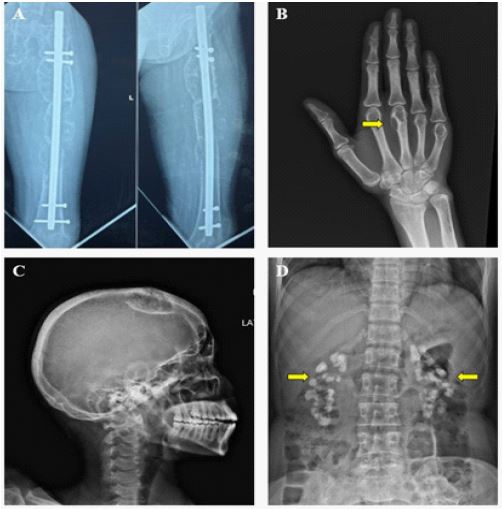
A 29-year-old woman with no known medical history presented with a one-year-old pathological fracture of her left femur following a trivial fall at her residence. Initially treated with an intramedullary nail, she complained of difficulty in walking and multiple bony aches. Physical examination revealed cachexia, multiple bony tender points, and bony swelling over her parietal bone. Sequential x-rays of her femur revealed thinning of cortices, generalized osteopenia, and scalloping of the medial femoral cortex. The latest radiograph (Figure 1, Panel A) showed diffuse cystic enlargement of the midshaft femur with multiple septae, a thinned-out cortex, diffuse osteopenia, and a loosened implant. A skeletal survey was performed which revealed the following features (Figure 1): Panel B: Thinning of metacarpal head cortex with a cystic enlargement (yellow arrow) classically named “osteitis fibrosa cystica/Browns tumor”; Panel C: skull radiograph with a cystic enlargement of the parietal bone with sclerotic margins and generalized osteopenia; Panel D: Multiple calcifications (yellow arrow) in both kidneys (nephrocalcinosis). Ultrasonography of the abdomen showed chronic calculous cholecystitis and bilateral medullary nephrocalcinosis. Biochemistry was notable as serum calcium was 14.1 mg/dl [reference 8.6 to 10.3], serum phosphorous was 1.8A 29-year-old woman with no known medical history presented with a one-year-old pathological fracture of her left femur following a trivial fall at her residence. Initially treated with an intramedullary nail, she complained of difficulty in walking and multiple bony aches. Physical examination revealed cachexia, multiple bony tender points, and bony swelling over her parietal bone. Sequential x-rays of her femur revealed thinning of cortices, generalized osteopenia, and scalloping of the medial femoral cortex. The latest radiograph (Figure 1, Panel A) showed diffuse cystic enlargement of the midshaft femur with multiple septae, a thinned-out cortex, diffuse osteopenia, and a loosened implant. A skeletal survey was performed which revealed the following features (Figure 1): Panel B: Thinning of metacarpal head cortex with a cystic enlargement (yellow arrow) classically named “osteitis fibrosa cystica/Browns tumor”; Panel C: skull radiograph with a cystic enlargement of the parietal bone with sclerotic margins and generalized osteopenia; Panel D: Multiple calcifications (yellow arrow) in both kidneys (nephrocalcinosis). Ultrasonography of the abdomen showed chronic calculous cholecystitis and bilateral medullary nephrocalcinosis. Biochemistry was notable as serum calcium was 14.1 mg/dl [reference 8.6 to 10.3], serum phosphorous was 1.8A 29-year-old woman with no known medical history presented with a one-year-old pathological fracture of her left femur following a trivial fall at her residence. Initially treated with an intramedullary nail, she complained of difficulty in walking and multiple bony aches. Physical examination revealed cachexia, multiple bony tender points, and bony swelling over her parietal bone. Sequential x-rays of her femur revealed thinning of cortices, generalized osteopenia, and scalloping of the medial femoral cortex. The latest radiograph (Figure 1, Panel A) showed diffuse cystic enlargement of the midshaft femur with multiple septae, a thinned-out cortex, diffuse osteopenia, and a loosened implant. A skeletal survey was performed which revealed the following features (Figure 1): Panel B: Thinning of metacarpal head cortex with a cystic enlargement (yellow arrow) classically named “osteitis fibrosa cystica/Browns tumor”; Panel C: skull radiograph with a cystic enlargement of the parietal bone with sclerotic margins and generalized osteopenia; Panel D: Multiple calcifications (yellow arrow) in both kidneys (nephrocalcinosis). Ultrasonography of the abdomen showed chronic calculous cholecystitis and bilateral medullary nephrocalcinosis. Biochemistry was notable as serum calcium was 14.1 mg/dl [reference 8.6 to 10.3], serum phosphorous was 1.8 mg/dl [reference 2.5 to 4.5], serum parathyroid hormone was 1004.4 pg/ml [reference 15 to 65], serum Alkaline phosphatase was 497 U/L [reference 35 to 104] and the 24 h urinary calcium was 455 mg [reference 100 to 300]. A diagnosis of primary hyperparathyroidism was made, confirmed by a right-sided parathyroid adenoma measuring around 0.8 x 0.8 x 0.6 cm on ultrasound of the neck and Tc-99m Sestamibi scan (Figure 2).

Discussion
Primary Hyperthyroidism (PHPT) is characterized by hypercalcemia and increased Parathyroid Hormone (PTH) levels in the bone. Parathyroid adenoma comprises 90% of all primary hyperparathyroidism patients and the remaining parathyroid hyperplasia [1]. PTH directly stimulates osteoclasts directly through its receptors and RANK-L and M-CSF synthesis and stimulates bone resorption. Excessive PTH levels lead to increased bone resorption from cortical bone and consequently increased calcium levels. This leads to areas of focal excessive bone resorption leading to cyst formation and replacement with fibrous tissue classically called osteitis fibrosa cystica or Brown tumor of the bone [2]. The other skeletal features include subperiosteal resorption of bone, tapering of small bones, and salt and pepper appearance of the skull [2]. Other features include nephrocalcinosis, nephrolithiasis, constipation, muscle weakness, and hypertension [3]. Hence the classical description is “the disease of stones, bones, and groans”. Laboratory tests in PHPT denote increased serum calcium levels, increased PTH levels and reduced serum phosphorous levels, and increased urinary calcium. Along with the radiography, the Technitium-99 Sestamibi scan is specific to diagnose parathyroid adenoma/hyperplasia [4]. Treatment of PHPT is by complete or partial parathyroidectomy and a successful surgery results in permanent normalization of calcium levels and improvement of bone mineral density [5].
Declarations
Conflicts of interest: Nil.
Research involving human participants and/or animals: Nil.
Informed consent: Informed consent was taken from the patient for this publication.
Funding: No funding was received to assist with the preparation of this manuscript. The authors have no relevant financial or non-financial interests to disclose.
References
- Walker MD, Bilezikian JP. Primary Hyperparathyroidism. In: Feingold KR, Anawalt B, Blackman MR, Boyce A, Chrousos G, Corpas E, et al., editors. Endotext. South Dartmouth (MA): MDText.com, Inc.; 2000.
- Bennett J, Suliburk JW, Morón FE. Osseous Manifestations of Primary Hyperparathyroidism: Imaging Findings. International Journal of Endocrinology. 2020; 2020: e3146535.
- Lin X, Fan Y, Zhang Z, Yue H. Clinical Characteristics of Primary Hyperparathyroidism: 15-Year Experience of 457 Patients in a Single Center in China. Frontiers in Endocrinology. 2021; 12.
- Naik M, Khan SR, Owusu D, Alsafi A, Palazzo F, et al. Contemporary Multimodality Imaging of Primary Hyperparathyroidism. RadioGraphics. 2022; 42: 841-60.
- Khan AA, Hanley DA, Rizzoli R, Bollerslev J, Young JEM, et al. Primary hyperparathyroidism: Review and recommendations on evaluation, diagnosis, and management. A Canadian and international consensus. Osteoporos Int. 2017; 28: 1-19.