
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 4
Duodeno-duodenal intussusception in a patient with chronic pancreatitis
Srikanth Kothalkar; Akash Mathur; Piyush Mishra; Ankur Yadav; Anshuman Elhence; Uday C Ghoshal*
Department of Gastroenterology, Sanjay Gandhi Postgraduate Institute of Medical Sciences, Lucknow 226014, India.
*Corresponding Author : Uday C Ghoshal
Department of Gastroenterology, Sanjay Gandhi Postgraduate Institute of Medical Sciences, Lucknow 226014, India.
Tel: 0522-2494405;
Email: udayghoshal@gmail.com
Received : Aug 04, 2023
Accepted : Aug 24, 2023
Published : Aug 31, 2023
Archived : www.jcimcr.org
Copyright : © Ghoshal UC (2023).
Keywords: Chronic pancreatitis; Frey’s procedure; Intussusception; Vomiting.
Acronyms: LPJ: Lateral pancreaticojejunostomy; CBD: Common bile duct; EGD: Esophagogastroduodenoscopy; CT: Computerised tomography; NJ: Naso-jejunal tube.
Citation: Kothalkar S, Mathur A, Mishra P, Yadav A, Ghosal UC. Duodeno-duodenal intussusception in a patient with chronic pancreatitis. J Clin Images Med Case Rep. 2023; 4(8): 2571.
Description
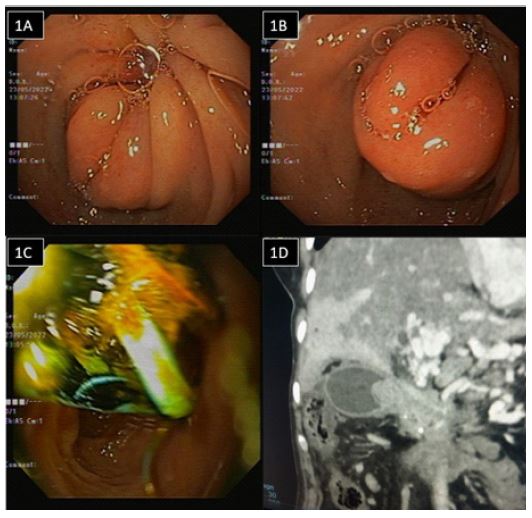
A 53-y old lady with chronic pancreatitis underwent a Frey’s procedure and Lateral Pancreaticojejunostomy (LPJ) in 2016. However, four years after the surgery, she developed a lower Common Bile Duct (CBD) stricture and was on endotherapy for the same, with currently four plastic stents in situ. On presentation, she had recurrent post-meal bilious vomiting, approximately 15 bouts a day, loss of appetite, retrosternal burning sensation and a localised abdomen swelling. On examination, she had epigastric fullness with a BMI of 14.7 Kg/m2. On Esophagogastroduodenoscopy (EGD), mucosal invagination was seen in the first part of the duodenum, suggestive of duodeno-duodenal intussusception, and the scope was negotiated across with difficulty into the second part of the duodenum (Figure 1A, B and C). A triphasic Computerised Tomography (CT) scan showed CBD stents in situ, atrophic pancreas and an ill-defined soft tissue in the region of the pancreatic head; also, the duodenum was thickened with doudeno-duodenal intussusception with upstream dilated stomach (Figure 1D). Tumor marker CA 19-9 was >1200 U/ml (Normal 0-37 U/ml). For gastric outlet obstruction due to duodenal intussusception, a Nasojejunal tube (NJ) was placed to maintain nutrition. Given the high suspicion of pancreatic malignancy and duodeno-duodenal intussusception, she was planned for definitive surgical management.
Duodeno-duodenal intussusception is characterised by the distal invagination of a segment of the duodenum into the duodenum itself [1]. This condition is rare because of the retroperitoneal fixation of the duodenum [2]. Only a few cases have been described previously in the literature. One patient developed duodeno-duodenal intussusception three months after Frey’s procedure and was managed by re-exploration [3]. A series of three cases from India describes gastric outlet obstruction with moderate to severe abdominal pain as the presentation in all these cases; our patient, however, only had mild pain abdomen [4]. The exact mechanism of duodeno-duodenal intussusception is unknown; it has been postulated that any lesion in the duodenal wall or irritant within the lumen that may alter normal peristaltic activity can initiate an invagination of the proximal bowel into the distal bowel. The lead point for this condition could be a polyp, malignant growth or an inflammatory mass.
Declarations
Conflict of interest: None of the other authors has any conflict of interest to declare concerning this paper.
Funding: None.
References
- Loo G, Mohamad Abu Zeid W, Lim S, Ismail A. Rare presentation of idiopathic duodenoduodenal intussusception. The Annals of the Royal College of Surgeons of England. 2017; 99.
- Guo Y, Liu B, Pan Z, et al. Acute duodenal obstruction secondary to intussusception caused by the duodenal diverticulum: A case report. BMC Gastroenterol. 2020; 20: 234.
- Mohsina S, Sureshkumar S, Sreenath GS, Kate V. Gastric outlet obstruction and intussusception following Frey’s procedure in a patient with chronic pancreatitis - A case report. J Mahatma Gandhi Inst Med Sci. 2018; 23: 98-100.
- Pradhan D, Kaur N, Nagi B. Duodenoduodenal intussusception: Report of three challenging cases with literature review. J Can Res Ther. 2015; 11: 1031.