
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 4
Hampton’s hump: An unusual radiological sign of pulmonary embolism
Chiu-Shih Cheng1; Chang-Hsien Ou2
1Department of Medical Imaging, E-Da Hospital, I-Shou University, No.1, Yida Road, Jiaosu Village, Yanchao District, Kaohsiung City 82445, Taiwan.
2Division of Neuroradiology, E-Da Hospital, I-Shou University, Kaohsiung City, Taiwan.
*Corresponding Author : Chiu-Shih Cheng
Department of Medical Imaging, E-Da Hospital, I-Shou University, No.1, Yida Road, Jiaosu Village, Yanchao District, Kaohsiung City 82445, Taiwan.
Email: csc109167@gmail.com
Received : Aug 08, 2023
Accepted : Aug 25, 2023
Published : Sep 01, 2023
Archived : www.jcimcr.org
Copyright : © Chiu-Shih C (2023).
Abstract
Hampton’s hump is a peripheral dome-shaped, opacification abutting the pleura, signifying pulmonary infarction distal to a pulmonary embolism. We report a case of pulmonary embolism that presented with the Hampton’s hump sign on a chest X-ray, which is an unusual yet moderately specific indicator for diagnosing pulmonary embolism.
Keywords: Hampton’s hump; Pulmonary embolism.
Citation: Chiu-Shih C, Chang-Hsien O. Hampton’s Hump: An unusual radiological sign of pulmonary embolism. J Clin Images Med Case Rep. 2023; 4(9): 2573.
Description
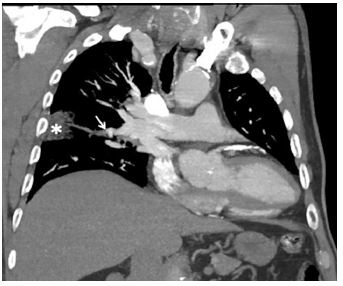
70-year-old male patient presented to the emergency department, complaining of right-sided chest pain persisting for the past two days. Notably, there were no significant underlying health conditions identified during the assessment. The physical examination did not reveal any remarkable findings. A chest radiograph showed dome-shaped, pleural based opacity in right middle lung field, consistent with Hampton’s hump (a white arrow in Figure 1), a finding that aroused concern about pulmonary embolism. The Electrocardiogram (ECG) did not show any abnormalities. The only abnormal blood test reported was a slightly elevated D-dimer of 4 mg/l (< 0.5 mg/l). Subsequent evaluation with a Computed Tomography (CT) pulmonary angiogram exhibited a filling defect within the segmental branch of the right middle lobe pulmonary artery (a white arrow in Figure 2). Additionally, a wedge-shaped ground glass change was observed in the lateral segment of the right middle lobe (an asterisk in Figure 2). These findings conclusively confirmed a diagnosis of pulmonary embolism with distal pulmonary infarction. It is noteworthy that Hampton’s hump, a seldom-seen radiographic indicator, is associated with pulmonary embolism. While the presence of a Hampton’s hump demonstrates a high degree of specificity (82%) for diagnosing pulmonary embolism, its sensitivity is relatively low (22%) [1-3]. Following treatment with heparin, the patient was discharged with a six-month anticoagulation regimen.

Declarations
Conflict of interests: No conflicts of interest.
Funding statement: All authors have no funding source to declare.
References
- Hampton AO, Benjamin L Castleman. “Correlation of postmortem chest teleroentgenograms with autopsy findings with special reference to pulmonary embolism and infarction.” 1940.
- Worsley DF, Alavi A, Aronchick JM, Chen JT, Greenspan RH, et al. Chest radiographic findings in patients with acute pulmonary embolism: observations from the PIOPED Study. Radiology. 1993; 189: 133-6.
- Han D, Lee KS, Franquet T, Müller NL, Kim TS, et al. Thrombotic and nonthrombotic pulmonary arterial embolism: Spectrum of imaging findings. Radiographics.