
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Disseminated tuberculosis in a patient with former history of MIS-C: Case report and review of the literature
Muntean Liviu1,2; Falup-Perucariu Oana1,2*; Atanasiu Denisa2; Poinareanu Ionut3,4,5; Mitrica Maria1,2; Papa Adrian1,2
1Faculty of Medicine, Transilvania University Brasov, Romania.
2Clinical Children’s Hospital of Brasov, Romania.
3Faculty of Medicine, University Ovidius Constanta, Romania.
4Faculty of Materials Science and Engineering, Transilvania University Brasov, Romania.
5Municipal Hospital of Sacele, Brasov, Romania.
*Corresponding Author : Falup-Perucariu Oana
Faculty of Medicine, Transilvania University Brasov, Romania.
Email: oanafp@yahoo.co.uk
Received : Aug 03, 2023
Accepted : Aug 28, 2023
Published : Sep 04, 2023
Archived : www.jcimcr.org
Copyright : © Oana FP (2023).
Abstract
Tuberculosis still remains a major health problem in our country. Young children and infants suffer more extra-pulmonary and disseminated TB. Diagnosis of this condition in this age group is usually difficult because of non-specific symptoms.
We present an 8-month-old infant with a history of SARS-CoV2 infection and MIS-C, initially admitted for a abscess in the left thigh, purulent secretions were positive for BK. After persistence of fever, CT scan revealed multiple osteolitic lesions with disseminated osteomyelitis. Confirmation of BK from gastric secretion was obtained and after surgical drainage of the largest bone lesion, medical treatment for BK was initiated (HRZE). The patient had an unfavourable evolution with pancytopenia, pulmonary insufficiency and eventually the patient succumbed to the disease 25 days after hospitalization.
Autopsy revealed disseminated TB with lesion involving the liver, spleen, bones and lungs.
Due to the MIS-C diagnosis, the patient was treated with high doses of methylprednisolone before admission, that could have triggered the disease.
There are currently no reported cases of disseminated TB after MIS-C in infants. Even though the incidence of TB has decreased in our country, clinicians should still consider a possible latent TB before prescribing corticotherapy in high doses and for long periods.
Keywords: Pediatric disseminated tuberculosis; Pediatric tuberculous osteomyelitis; Mycobacterium tuberculosis; Tuberculosis after MIS-C; Corticosteroids in tuberculosis.
Citation: Liviu M, Oana FP, Denisa A, Ionut P, Maria M, et al. Disseminated tuberculosis in a patient with former history of MIS-C: Case report and review of the literature. J Clin Images Med Case Rep. 2023; 4(9): 2576.
Introduction
Tuberculosis is an infectious disease caused most frequent by Mycobacterium tuberculosis and less common by Mycobacterium bovis, which typically occurs in immunocompromised patients [1]. Tuberculous osteomyelitis may occur in 10 to 35 percent of cases of extrapulmonary tuberculosis and overall, for almost 2 percent of all cases of TB [2].
The incidence of tuberculosis in Romania gradually decreased from 158 cases per 100,000 people in 2002 to 45 cases per 100,000 people in 2021 [3]. However, it still remains a major public health problem in our country by having the highest TB incidence in the European Union [4]. In 2015, an analysis of TB cases in our country was carried out and it found a prevalence of 0.02% in children between 0-4 years and a prevalence of 0.03% in children between 5-14 years. In the same year, the incidence in children aged 0-4 was 24 per 100,000 and in those aged 5-14 it was 21 per 100,000 [5].
The disease has been reported to affect all bones in the body, but most frequent it affects the spines, followed by the hip, elbow, femur, tibia, fibula, small bones of the hands and feet, rarely affecting the shoulder or metatarsal bones [6,7].
Usually, the clinical signs are characterized by localized pain and swelling. These may precede inflammatory signs and radiological changes by weeks or months. Unspecific symptoms such as fever and weight loss are less common [6].
Young children, especially infants suffer more extrapulmonary and disseminated TB than adults, but diagnosis is more difficult at this age group due to non-specific or complete absence of signs and symptoms. Bacteriological diagnosis has a low specificity, because collected pathological products are paucibacillary and often it is not possible to obtain good-quality sputum. Treatment is challenging due to the lack of pediatric drug formulations and challenges in toxicity monitoring [8].
Case presentation
We present a case of an 8-month-old male infant, with a birthweight of 3980 grams and good newborn adaptation. He received BCG vaccine in the maternity. At the age of 4-months he was confirmed with SARS-CoV-2 infection and one month later he was diagnosed with MIS-C. At the age of 6-months he received DTaP and anti-pneumococcal vaccine at his family doctor according to the NIP. He was transferred to our hospital from a territorial hospital due to fever with an onset of 12 days. Until admittance at our hospital, he received treatment with meropenem and vancomycin for 7 days and methylprednisolone sodium succinate for 5 days.
At admission, the infant’s weight was 8 kilograms, his general state was poor and had pale skin. Upon inspection of the left lower limb, we noticed a swelling in the middle third of the left thigh antero-lateral face. Palpation revealed a well-defined tumorous formation, which did not present any of the Celsius signs (Figure 1).
Initial laboratory tests revealed microcytic hypochromic anemia with Hb = 7.2 g/dL (N = 11.4-14.0 g/dL), VEM=64.2 fL (N = 70-89 fL), HEM = 20.5 pg (N = 25-30 pg), lymphopenia 1.3*103/μL (N = 4-13.5 x 103/μL), severe biological inflammatory syndrome with a C reactive protein of 35.91 mg/dL (N = 0-1 mg/ dL), ESR 60 mm/h (N = 0-10 mm/h) and fibrinogen 657 mg/dL (N = 180-450 mg/dL). The SARS-CoV-2 IgG and IgM were both negative.


Presumptive diagnosis was left thigh abscess and sepsis. It was decided that treatment should be continued with meropenem and vancomycin.
Puncture and aspiration of purulent secretions were performed under general anesthesia. The pathological sample was taken to the laboratory for cultures (including for BK due to the persistent fever under antibiotic treatment). The patient’s evolution was initially favorable, with a decrease in CRP, but after 2 days his condition worsened, with a progressive increase in inflammatory markers.
Soft tissue ultrasound revealed a collection image with adjacent edema and fluid fuzes along the muscle fibers on the left thigh, right above the puncture site. The abdominal and thoracic ultrasound did not reveal peritoneal fluid nor pleural fluid and the transfontanellar ultrasound was also normal.
Thorax, abdomen and pelvis contrast CT-scan was performed and revealed multiple osteolytic lesions typical image for septic bone dissemination, left thigh abscess and bilateral pulmonary septic dissemination. The diagnosis was left femur and left iliac wing osteomyelitis (Figure 2).
Surgery was performed with osteotomy of the left iliac wing with drainage. Purulent secretions and bone cellular detritus were removed and a suction drainage tube was placed at the level of the bone abscess in the left iliac wing.
The GeneXpert test from gastric lavage and purulent secretions from left thigh abscess were intensely positive (+++) for Mycobacterium tuberculosis sensitive to isoniazid and rifampin. No other Gram positive or negative bacteria were identified. Epidemiological investigation was carried out, but no case was detected in his contacts.

Medical treatment consisted in administration of fluids, amino acids, isoniazid (H), Rifampin (R), Pyrazinamide (Z) and ethambutol (E) (HRZE), antibiotherapy (clindamycin, linezolid, further on replaced by piperacillin-tazobactam), dexamethasone, immunoglobulin, human albumin, furosemide, vitamin B6 and vitamin D3. The corticosteroid therapy was stopped immediately after finding out the positive result for BK. The patient also received blood and platelet transfusions, due to pancytopenia especially given by severe thrombocytopenia.
The patient’s general condition progressively worsened, despite treatment. He became oxygen dependent, tachycardic, febrile, and his pulmonary state worsened. Later on, he presented a pathological fracture of the left humeral neck (Figure 3).
He was intubated and mechanical ventilated. Acid-base parameters indicated severe respiratory acidosis while the other laboratory tests showed persistent moderate anemia Hb = 7.4 g/dL (N = 11.4-14.0 g/dL), severe thrombocytopenia 38*103/μL (N = 150-400 x 103/μL), high levels of CRP = 27.24 mg/dL (N = 0-1 mg/dL) and procalcitonin = 3.5 ng/mL (N = 0-0.5 ng/mL), hyperferritinemia = 1472 μg/L (N=10-120 μg/L) and hypoalbuminemia = 3.3 g/dL (N = 3.9-5.1 g/dL). He presented cardiac arrest through asystole, resuscitation maneuvers were ineffective and death was declared on the 25th day of hospitalization.
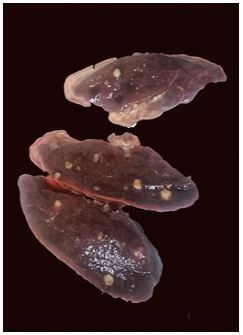
An autopsy was performed that revealed: cerebral petechiae, polyserositis (due to the presence of pericardial, pleural and peritoneal fluid), bilateral pulmonary hemorrhage, miliary nodular lesions (more evident on the right lung), erosions of the gastric and intestinal mucosae, hepatomegaly and liver dystrophy, miliary lesions at the level of the liver (Figure 4).

and spleen, shock kidneys, osteolytic lesions at the level of the skull, vertebrae, ribs, iliac bones, skin petechiae and ulceration in the upper third of the left humerus. The post-mortem diagnosis was disseminated tuberculosis.
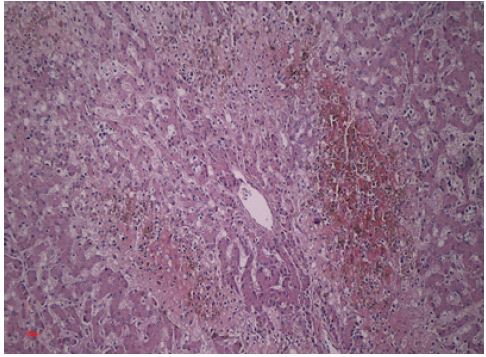
The microscopic examination (Hematoxylin-Eosin 10x) revealed a liver tissue with the presence of areas of necrosis, lymphocytic inflammatory infiltrate and biliary atrophic structures. Peripherally, lobular hepatocytes with optically empty intracytoplasmic vacuoles were identified. This aspect advocates for an infiltrative-exudative form of tuberculosis (Figure 5).
The hepatic central vein was also observed flanked by abscessed areas due to superinfection and lesions of liver suffering due to its dilated appearance (Figure 6).
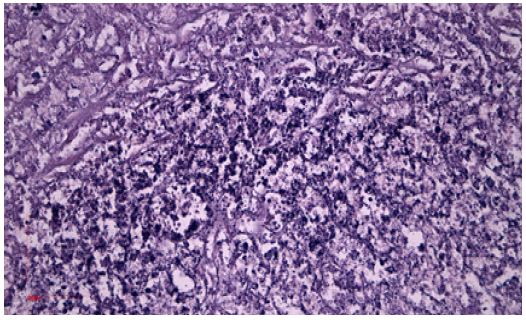
Table 1: Cases from literature with TB related to MIS-C.
| Authors | Case description | Comments |
|---|---|---|
| Morel, Z., Suarez, R., Avalos, E., Velázquez, S., Martínez, F., Lezcano, V., Astigarraga, N., Ghezzi, C. et al. [9] |
A 7-year-old boy with a history of COVID-19 in the family had bone-marrow TB, which was responsive to tocilizumab treatment. | Lab tests revealed hyperferritinemia, high levels of D-dimers, CRP and IL-6. Doppler’s echocardiography showed cardiac abnormalities. |
| Almatrafi, M.A., Awad, K., Alsahaf, N., Tayeb, S., Alharthi, A., Rabie, N., Fadag, R., Alwafi, H. et al. [10] | A 17-year-old male patient with COVID-19 five weeks ago was diagnosed with TB lymphadenitis and Pott’s disease. | The patient presented leukocytosis with lymphopenia. CT scan revealed multiple lymphadenopathies and bony lytic lesion in T10 and T12. Ultrasound showed multiple caseating granulomas. |
| Khataniar, H., Diya S., Lalitha, A.V. [11] | A 14-year-old male patient with positive IgG SARS-CoV-2 antibodies had latent disseminated TB (meningitis, peritonitis, pulmonary) | The patient had TB meningitis and hydrocephalus in early childhood which were treated with VP shunt. |
| Tripathy, V., Bela V. [12] | An 11-year-old female patient with positive SARS-CoV-2 IgG antibodies had disseminated TB. She had positive sputum with rifampicin resistance and positive GeneXpert from urine. | Imaging revealed miliary shadows, ring-enhancing lesions with perilesional oedema, necrotic mediastinal limphadenopathy, bilateral bulky kidneys with cortical hypodense areas. Ophtalmic exam showed multiple choroid tubercles. |
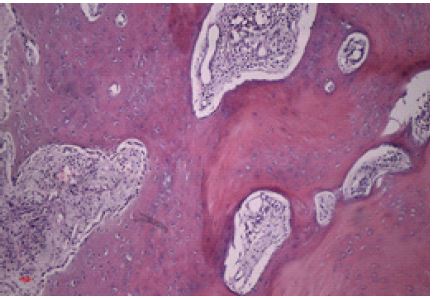
Bone tissue fragments and hematogenous marrow had a normal appearance (Figure 7).
Hepatic tissue (Hematoxylin-Eosin 400x) Bacterial colonies that produced superinfection in the liver (Figure 8).
The images were captured using a camera included in an optical microscope with polarized light and phase contrast Motic Panthera 2.1.3.
Discussion and review of literature
We performed a search in the Google Scholar and PubMed databases and extracted case reports of pediatric patients who were diagnosed with tuberculosis after infection with SARS-CoV2 (Table 1).
No studies have been found to prove that DTaP and anti-pneumococcal vaccination that the patient received at 6-month old could have an influence on the development of TB.
Our patient had MIS-C and he was under treatment with methylprednisolone sodium succinate before the admission to our hospital, therefore this can be considered a possible trigger for his disease. Corticosteroid therapy is not usually recommended because it can reactivate latent TB or even it may trigger the debut of TB [13].
Another study suggested that corticosteroids given early on when the viral load is low could cause immunosuppression, that can lead to secondary superinfections with other pathogens [14].
On the other hand, this type of treatment could have beneficial effects in some patients by their anti-inflammatory properties alongside with a reduction in systemic symptoms of TB, such as fever, weight loss, headache and chest pain [13].
One study was found in which the author claims that CD4+ T-cell depletion associated with COVID-19 may be implicated in the progression of LTBI to active TB [15].
MIS-C or Multisystem Inflammatory Syndrome in Children is a rare, but serious condition associated with COVID-19, which according to CDC is defined by presence of fever, severe illness requiring hospitalization or resulting in death, laboratory evidence of systemic inflammation (elevated CRP, ESR, procalcitonin), cardiovascular involvement (elevated troponin, NT-proBNP, D-dimers), hematologic manifestations (platelet count < 150,000 x 103/μL or lymphocyte count <1 x 103/μL), gastrointestinal and dermatological problems, evidence of exposure to SARS-CoV-2 virus and no other alternative plausible diagnoses. All these signs should appear in patients under the age of 21. [16] Our patient had MIS-C defined as CDC prior to admittance at our hospital, manifested by prolonged fever and history of COVID-19 at 4 months old. Later on, we had the evidence of high inflammatory markers (CRP, ESR), thrombocytopenia, lymphopenia, distended abdomen.
Our patient was in a category of high risk of getting TB by having a small age, coming from an endemic area and having the history of MIS-C, all these factors being aggravated by corticosteroid treatment.
There are no reported cases of disseminated TB after MIS-C in infants. A few articles with TB - COVID-19 co-infection were found, but those were excluded from this study. However apparently there is higher incidence of male cases in published cases. Several studies also revealed a preponderance of TB infection in males.
As can be seen in Morel’s study [9], their patient also received treatment with vancomycin and corticosteroids, but only responded once tocilizumab treatment was initiated. Several other studies demonstrated that monoclonal antibodies can improve the evolution of TB. If the tuberculosis is disseminated, it is recommended to administer from the very beginning monoclonal antibodies.
However, our patient did not receive tocilizumab because this drug is not part of our TB treatment protocol at this particular age.
Conclusion
Although the incidence of tuberculosis in Romania has decreased in the last years, it still remains a major problem. Clinicians should be paying attention especially among children who have gone through a SARS-CoV-2 infection with clinical and paraclinical evidence of MIS-C, because this could influence the subsequent evolution of TB.
Even if we do not have evidence that that DTaP and anti-pneumococcal vaccination directly caused TB in our particular case, patients which received corticosteroid therapy should postpone vaccination. In cases where we suspect a TB infection, it is recommended to immediately stop corticosteroids until the diagnosis is confirmed.
Monoclonal antibodies could be a future therapy among children with disseminated TB, but more studies in this direction are needed.
References
- Sambyal SS, Dinkar AD, Jayam C, Singh BP. Primary tuberculous osteomyelitis of the mandible in a 3-year-old child. Case Reports. 2016; bcr2016216854.
- Singh A, Chatterjee P, Pai MC, Chacko RT. Tuberculous osteomyelitis of the scapula masquerading as metastasis. Journal of Radiology Case Reports. 2009; 3: 27-31.
- Romania - Incidence of tuberculosis https: //knoema.com/atlas/Romania/Incidence-of-tuberculosis
- Golli AL, Niţu MF, Turcu F, Popescu M, Ciobanu-Mitrache L, et al. Tuberculosis remains a public health problem in Romania. The International Journal of Tuberculosis and Lung Disease. 2019; 23: 226-231.
- Socaci A, Mahler-Boca B, Chiotan DI, Popescu G, Stefan M, et al. The Tuberculosis Epidemic in Romania: TB Allocative Efficiency Model Findings and Recommendations. 2019.
- Yuen MC, Tung WK. An uncommon cause of foot ulcer: tuberculous osteomyelitis, Emergency Medicine Journal. 2001; 18: 140-141.
- Agarwal A. Paediatric osteoarticular tuberculosis: A review. Journal of Clinical Orthopaedics and trauma. 2020; 11: 202-207.
- Loeffler AM. Pediatric tuberculosis. Seminars in respiratory infections. 2003; 18: 272-291.
- Morel Z, Suarez R, Avalos E, Velázquez S, Martínez F, et al. Multisystemic inflammatory syndrome related to COVID-19, with latent tuberculosis in bone marrow, and satisfactory response to tocilizumab, in a 7-year-old boy. Reumatismo. 2021; 73.
- Almatrafi MA, Awad K, Alsahaf N, Tayeb S, Alharthi A, et al. Disseminated Tuberculosis Post COVID-19 Infection: A Case Report. Cureus. 2022; 14.
- Khataniar H, Diya S, Lalitha AV. Disseminated TB in the Setting of COVID-19 Infection- a Cause or a Consequence? Pediatrics. 2022; 149: 401-401
- Tripathy V, Bela V. Development of Disseminated Drug resistant Tuberculosis in an Immunocompetent Patient after COVID-19 Infection. Postgraduate Journal of Pediatrics and Adolescent Medicine. 2022; 1: 30-33.
- Cisneros JR, Murray KM. Corticosteroids in tuberculosis. Annals of Pharmacotherapy. 1996; 30: 1298-1303.
- Gopalaswamy R, Subbian S. Corticosteroids for COVID-19 therapy: potential implications on tuberculosis. International journal of molecular sciences. 2021; 22: 3773.
- Khayat M, Fan H, Vali Y. COVID-19 promoting the development of active tuberculosis in a patient with latent tuberculosis infection: a case report. Respiratory Medicine Case Reports. 2021; 32: 101344.
- CDC and WHO case definitions of multisystem inflammatory syndrome in children https: //www.uptodate.com/contents/image?imageKey=PEDS%2F128201