
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Volkmann’s ischemic contracture with impaired vascularity managed by minimally invasive soft tissue release and capsulotomy: A rehabilitation perspective
Jaya Das; Badarinath Athani; Anindya Debnath*
Department of Physical Medicine and Rehabilitation, St John’s Medical College, Bengaluru, India.
*Corresponding Author : Anindya Debnath
Department of Physical Medicine and Rehabilitation, St John’s Medical College, Bengaluru, India.
Email: anindyadebnath@gmail.com
Received : Aug 04, 2023
Accepted : Aug 29, 2023
Published : Sep 05, 2023
Archived : www.jcimcr.org
Copyright : © Debnath A (2023).
Abstract
Volkmann’s ischemic leg contracture is severe and debilitating, arising from prolonged ischemia of the lower limb musculature. This condition, also known as Volkmann’s syndrome or Volkmann’s ischemic contracture, occurs because of reduced blood supply to the muscles and nerves, leading to irreversible tissue damage and subsequent contracture formation. This article provides a comprehensive overview of one such chronic case associated with this distressing medical condition resulting in significant functional impairment and its successful operative rehabilitation approach.
The pathogenesis of Volkmann’s ischemic contracture (VIC) involves a cascade of events initiated by prolonged arterial occlusion, leading to cellular hypoxia, metabolic derangements, and the release of toxic metabolites, culminating in irreversible tissue damage and fibrosis. VIC of leg, if not treated early, can lead to deformity of foot and ankle complex.
Determination of the exact deformities of foot and ankle is crucial in deciding the surgical correction needed. In our case, he presented with left equino-varus deformities and underwent soft tissue procedure followed by physical therapy, early mobilization with appropriate orthotic and footwear.
The rehabilitation approach of chronic VIC of leg is a multifaceted process that involves careful assessment, monitoring, rehabilitation, and long-term follow-up. In this case, surgery and post-operative rehabilitation was uneventful and he continues to sustain the functional improvement on follow up.
Keywords: VIC; Equino-varus; Tenotomy; Capsulotomy.
Citation: Das J, Athani B, Debnath A. Volkmann’s ischemic contracture with impaired vascularity managed by minimally invasive soft tissue release and capsulotomy: A rehabilitation perspective. J Clin Images Med Case Rep. 2023; 4(9): 2578.
Introduction
Volkmann’s ischemic contracture of leg is not a common occurrence and usually follows compartment syndrome i.e., ischemic insult to the leg compartment resulting from direct or indirect trauma.
Established surgical protocols are performed in a stepwise fashion, to include: [1] Release of residual or secondary nerve compression, [2] release of fixed contractures, using infarct excision, myotendinous lengthening, muscle recession, or tenotomy, [3] tendon transfers or arthrodesis to increase function, and [4] ostectomy or amputation for severe, refractory deformities. Surgical decision making with methodical rehabilitation planning is key to achieve adequate functional gain.
Case presentation
A 26-year-old, male, from Bangladesh, who is a driver by profession, was well until February 2019, when he allegedly met with a road traffic accident. He was immediately taken to a hospital nearby. Imaging showed left hip comminuted fracture (left acetabular and iliac bone) and was managed conservatively with left hip plaster and leg traction. Post traction he had swelling of his left leg and was diagnosed as VIC of leg. He was managed with analgesics and antibiotics. Post discharge, he started ambulating after 1 month with minimum weight bearing. Gradually he developed deformity in his left foot with a wound on the dorsum of the foot with persistent discharge.
On presentation, he was completely independent for mobility and all ADLs. He was continent for both bowel and bladder. He was ambulating with minimal weight bearing on left lower limb with bilateral elbow crutches and was admitted for deformity correction and further rehabilitation.
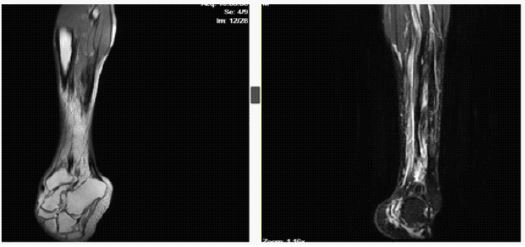
He was accurately assessed by the rehabilitation team. Left lower limb arterial doppler showed low velocity biphasic flow in distal anterior tibial artery. MRI of left leg showed Volume loss secondary to muscle atrophy involving all three muscle compartments of mid and distal 1/3rd of left leg. Surgical intervention was planned after explaining the guarded prognosis. The following procedures were done to achieve proper correction-
i) Posterior release- Tendo Achilles lengthening + posterior capsulotomy of ankle and subtalar joint.
ii) Medial release- Tibialis posterior, flexor digitorum longus, flexor hallucis longus tenotomy.
iii) Plantar release- plantar fasciotomy, abductor hallucis release
iv) Release of all fibrous bands
The operation was done with tourniquet for 1 hour. Post operatively, the patient was put on a well-padded plaster of Paris cast in 5-degree dorsiflexion for 15 days. After that suture removal was done followed by manipulation and Arte walking cast for 6 weeks. Almost full correction was achieved on removal of the Arte cast. The patient was comfortable with molded insole and gait was near normal.
2nd stage of operation is deferred as of now.

Discussion
Volkmann’s syndrome or Volkmann’s ischemic contracture, occurs as a result of reduced blood supply to the muscles and nerves, leading to irreversible tissue damage and subsequent contracture formation. Early recognition and prompt intervention are crucial to prevent long-term disability and functional impairment.
In a previous review article by Mark D. Santi [2], it mentions the challenges of severe deformities and step wise surgical correction for such deformities. He also mentions about the importance of a proper identification of the ischemic deformities of foot and ankle and the role of non-operative management in the form of physical therapy, corrective bracing and accommodative footwear.
Management of Volkmann’s ischemic contracture necessitates a multi-faceted approach. Advanced cases like in our case of Volkmann’s ischemic contracture required surgical intervention, to improve joint mobility and functionality. Post-surgical rehabilitation and long-term follow-up are essential to optimize the outcomes and prevent complications.
Early mobilization and physical therapy were the essential components of the post-surgery plan. Rehabilitation aims to prevent joint contractures, maintain muscle flexibility, and improve overall functional outcomes. Depending on the extent of contractures and joint involvement, the use of splints or orthotics may be beneficial. These aids help maintain proper limb alignment and prevent further contracture formation during the healing process.
In our case, he benefited with the soft tissue procedure followed by physical therapy and orthotic intervention and was able to resume daily activities with improved functional outcome.
A significant aspect of the post-surgery discussion is the patient’s functional outcomes and quality of life. Understanding the patient’s goals, limitations, and expectations allows healthcare providers to tailor the rehabilitation process to maximize independence and overall well-being.
Conclusion
The minimally invasive soft tissue procedure with custom molded shoe, done with meticulous rehabilitation decision making, has proven to be an excellent treatment modality for this case of VIC with impaired vascularity. The patient is walking without any mobility aid and currently has no other associated complaint. By implementing a collaborative and patient-centered approach, healthcare providers can optimize the patient’s recovery and strive for the best possible functional outcomes and quality of life.
Competing interests: No conflicts of interest.
Funding details: Nil.
References
- Lortat-Jacob A, Faivre M, Benoit J, Ramadier JO, Laurian C, et al. Les séquelles au pied du syndrome de Volkmann [Deformities of the feet after Volkmann’s ischemia in the lower limb (author’s transl)]. Rev Chir Orthop Reparatrice Appar Mot. 1981; 67: 617-24.
- Santi MD, Botte MJ. Volkmann’s ischemic contracture of the foot and ankle: Evaluation and treatment of established deformity. Foot Ankle Int. 1995; 16: 368-77.
- Zwipp H. Rekonstruktive Massnahmen am Fuss nach Kompartmentsyndrom [Reconstructive measures for the foot after compartment syndrome]. Unfallchirurg. 1991; 94: 274-9.
- Frink M, Hildebrand F, Krettek C, Brand J, Hankemeier S. Compartment syndrome of the lower leg and foot. Clin Orthop Relat Res. 2010; 468: 940-50.