
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Persistent left SVC: Can nephrologist use it for dialysis?
Prem P Varma1*; Mehak Singla2
1Department of Nephrology, Primus SuperSpecialty Hospital, New Delhi, India.
2Consultant Nephrologist, Primus SuperSpecialty Hospital, New Delhi, India.
*Corresponding Author : Prem Prakash Varma
Department of Nephrology, Primus SuperSpecialty Hospital, New Delhi, India.
Email: genvarmapp@gmail.com
Received : Aug 08, 2023
Accepted : Aug 30, 2023
Published : Sep 06, 2023
Archived : www.jcimcr.org
Copyright : © Varma PP (2023).
Abstract
Persistent left sided superior vena cava (PLSVC), though rare, is the most common congenital anomaly of thoracic venous circulation. Most of the times, it gets incidentally detected during left internal jugular venous hemodialysis catheter insertion. Whether to keep this catheter and give hemodialysis through this, is a debatable issue. We discuss a case where successful maintainence hemodialysis was given through PLSVC for seven months.
Citation: Varma PP, Singla M. Persistent left SVC: Can nephrologist use it for dialysis?. J Clin Images Med Case Rep. 2023; 4(9): 2580.
Introduction
Persistent Left Sided Superior Vena Cava (PLSVC) is encountered in 0.3% of healthy population and majority of times, it gets incidentally detected during a left sided internal jugular catheter insertion or during electrophysiological studies. There are couple of reports where after its accidental cannulation, dialysis has been continued for variable period of time. We report a case where PLSVC was incidentally detected after left sided cannulation of Internal jugular vein. Dialysis was successfully continued through this route for next seven months, till the catheter got thrombosed.
Case presentation
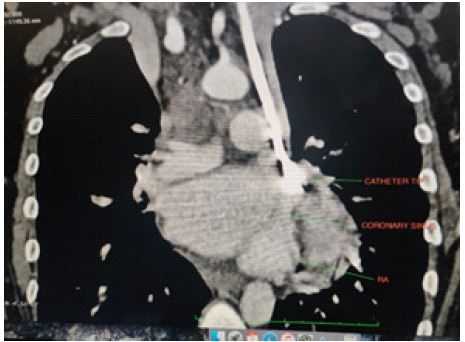
A 26-year-old lady on regular maintenance hemodialysis for basic disease IgA nephropathy, came to us for vascular access creation after her right IJV got thrombosed. She was on thrice a week dialysis for last 2 years and two attempts to make AV fistula had failed. An uneventful Left sided IJV catheterization was done. Surprisingly a check X-ray showed that catheter was lying on the left side of sternum (Figure 1). For fear of wrong cannulation into some other vessel, arterial blood gas analysis and echocardiography was done which suggested Left sided superior vena cava. A contrast enhanced CT confirmed the diagdiagnosis. It was draining into coronary sinus and eventually in right atrium (Figure 2). We started the dialysis through this catheter, initially keeping the blood flow rate of 200-250 ml/min and keeping a watch on hemodynamic compromise or arrhythmias. As there was no complication, blood flow rate was increased to 300 ml/min. Patient has been on thrice a week dialysis through this access for the last 7 months without any complication.

Discussion
PLSVC is the most common congenital anomaly of thoracic venous circulation encountered in 0.3-0.5% population and in 4.5% in those with congenital heart disease. It generally gets detected accidently during cannulation of left Internal jugular vein or during pacemaker placement. Majority of times (92%), it drains through coronary sinus into right atrium and rarely into left atrium [1-3]. Embryologically human left SVC originates in the third week of the embryonic period, and then the left anterior cardinal vena cava gradually atrophies and finally degenerates into the ligament of Marshall. If the degeneration is not complete, then the remains of a pipeline structure after birth is PLSVC. Based on anatomy, Schumer [4] classified SVC into 3 types. Type I, normal anatomy; Type II, only persistent left superior vena cava; Type IIIa, right and left superior vena cava with connection; Type IIIb, right and left superior vena cava without connection.
Based on the drainage characteristic, Zhu [5] classified PLSVC, into 4 types. Type A- PLSVC draining blood to the right atrium via coronary sinus, Type B- PLSVC draining blood to the right atrium via coronary sinus with partial right-to-left shunt, Type C- PLSVC drains blood to left atrium directly with right-to-left shunt and type D- PLSVC is directly connected to left pulmonary vein (coronary sinus absent)
Our case fits into Schummer’s Type III b class and based on drainage into Zhu’s Type A and this combination is the most common. Many workers have reported uneventful catheterization like in our case [1-3]. Most of the times PLSVC drains into right atrium through coronary sinus. Because of higher blood flow, sinus gets dilated and enlarged. An enlarged coronary sinus on echocardiography is a hint towards PLSVC. Due to coronary sinus stimulation by catheter, few cases of arrhythmia, angina, stroke and shock have been reported. If PLSVC drains into left atrium, there is usually a cardiac septal defect like atrial or ventricular. It can have dangerous outcome for patient, as there may be cyanosis and fear of systemic embolization.
Whether dialysis should be continued through PLSVC, is not an easy answer. If it is draining into Left atrium, dialysis is not possible. If it is draining into right atrium through coronary sinus, dialysis can be offered if there is no hemodynamic compromise/arrhythmia following catheter insertion and dialysis. It is suggested that to avoid irritation of coronary sinus, the catheter tip (which is normally placed in right atrium), should be placed at lower end of PLSVC as it is not possible to place it in right atrium and it is not advisable to place it in coronary sinus. As cardiac arrhythmias have been reported even after 2-3 sessions of dialysis, it is prudent to be aware of this possibility.
A check X-ray showing IJV catheter on left side of sternum, after left sided IJV cannulation may prompt nephrologist to remove the catheter fearing cannulation of an artery. However if fluoroscopy guided/real time ultrasonography guided cannulation is done, such fear gets obviated. Arterial blood gas analysis also removes fear of arterial cannulation. Catheter lying on left side of sternum should make one suspect of PLSVC and a dilated coronary sinus on echocardiography gives an additional hint. Echocardiography generally gives the diagnosis and CT angiography confirms the diagnosis. Cardiac catheterization is the gold standard for diagnosis of PLSVC, however to avoid invasive procedure thoracic enhanced CTA is an alternative [5-7].
He et al, on compilation of data, found 28 case reports of PLSVC among dialysis patients, 12 had tunneled cuffed catheter placement and 16 non-cuffed catheters. Dialysis has been performed in some of these patients for variable period of time (2-32 months) and few complications like angina, stroke, arrhythmias etc. have also been reported.
We are reporting the case to bring awareness among nephrologists (proceduralist) of this rare entity. Dilemma of continuing dialysis in such cases is not straight forward. We feel PLSVC can be used as vascular access (like in our case) provided it is providing adequate blood flow and is draining in coronary sinus and into right atrium. It is prudent to look for any complication like arrhythmias during initial dialysis sessions.
References
- Kute VB, Vanikar AV, Gumber MR, Shah PR, Goplani KR, et al. Hemodialysis through persistent left superior vena cava. Indian J Crit Care Med. 2011; 15: 40-42.
- Anvesh G, Raju SB, Rammurti S, Prasad K. Persistent left superior vena cava in a hemodialysis patient. Indian J Nephrol. 2018; 28: 317-319
- Lim TC, H’ng MW. Persistent left superior vena cava: A possible site for haemodialysis catheter placement. Singapore Med J. 2010; 51: e195-197.
- Schummer W, Schummer C, Fröber R. Persistent left superior vena cava and central venous catheter position: Clinical impact illustrated by four cases. Surg Radiol Anat. 2003; 25: 315-21.
- Zhu X. Basic Illustrations for Cardiac Surgery. 2nd ed. Beijing: Peking union medical college press. 2010; 257-64.
- Azizova A, Onder O, Arslan S. et al. Persistent left superior vena cava: linical importance and differential diagnoses. Insights Imaging. 2020; 11: 110.
- He H, Li B, Ma Y. et al. Catheterization in a patient with end-stage renal disease through persistent left superior vena cava: a rare case report and literature review. BMC Nephrol. 2019; 20: 202.