
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Research Article - Open Access, Volume 4
Implications of bacterial plaque in gingival overgrowth induced by orthodontic therapy
Alina Cristina Rădeanu1; Anca Mihaela Predescu2 ; Adelaida Georgiana Stanca3, Mihai Surpățeanu4; Elena Cristina Andrei5*; Oprea Valentin Bușu6
1PhD Student, Oro-Maxillo-Facial Surgery Doctor, Polyclinic from Craiova, Dolj, Romania.
2Faculty of Dentistry, University of Medicine and Pharmacy. Lecturer, Department of Histology, University of Medicine and Pharmacy, 200349 Craiova, Romania.
3Student, Faculty of Dentistry, University of Medicine and Pharmacy, 200349 Craiova, Romania.
4Department of Oro-Maxillo-Facial Surgery, University of Medicine and Pharmacy, 200349 Craiova, Romania.
5Faculty of Dentistry, University of Medicine and Pharmacy. Teaching Assistant, Department of Histology, University of Medicine and Pharmacy, 200349 Craiova, Romania.
6Teacher Training Department, University of Craiova, Romania.
*Corresponding Author : Elena Cristina Andrei
Department of Histology, University of Medicine and Pharmacy, 200349 Craiova, Romania.
Email: andreicristina@gmail.com
Received : Aug 09, 2023
Accepted : Aug 31, 2023
Published : Sep 07, 2023
Archived : www.jcimcr.org
Copyright : © Andrei EC (2023).
Abstract
Aim: To present clinical aspects of gingival overgrowth induced by orthodontic therapy and to evaluate the consequences of the presence of bacterial plaque during orthodontic treatment.
Methods: Our study included a number of 15 subjects diagnosed with gingival overgrowth due to orthodontic reasons. The subjects presented themselves at the Oro-Maxillo-Facial Surgery Clinic in the city of Craiova, Romania, complaining of gingival bleeding, functional and masticatory disorders, but also of an aesthetic nature. Each subject was given a file, anamnesis, general and local clinical examination and were entered into a database created in the Excel program that includes information related to sex, age group, occupation, systemic diseases, allergies, drug treatments or surgical, O’Leary Plaque Index, duration of orthodontic treatment, age of the gingival overgrowth lesion. The informed consent of each subject was obtained.
Results: The subjects are included the age group of 12-27 years. Our study highlighted the fact that gingival overgrowth induced by orthodontic therapy tends to affect more male subjects (73.3%) than female subjects (26.6%). All subjects were tested for allergy to metal alloys from which the dental appliances are made, but no subject showed hypersensitivity. For each subject we calculated the O’Leary Plaque Index and it can be seen that most subjects had a score between 40-59%, this being a percentage worryingly, the duration of orthodontic treatment varies between 2 months and 3 years, most subjects are included the category of more than 1 year, and the age of gingival overgrowth varies between one month and 6 months. At the same time, it was noticed that subjects who have had orthodontic appliances for more than a year that the gingival overgrowth has a generalized form, being much more severe. Gingival lesions are detected in the early stages, often because the subjects go for regular check-ups once a month.
Conclusion: Bacterial plaque significantly influences the evolution and severity of gingival overgrowth induced by orthodontic therapy. The dentist has the duty to educate the patient and draw his attention to the fact that during orthodontic treatment the hygiene rules are much more rigorous, because braces are elements that retain bacterial plaque and food debris. Currently, there are many attractive techniques for familiarizing children and adolescents with the rules of oral hygiene that can be performed both at home and in the doctor’s office. Access to the applications aimed at this topic installed on the smartphone bring a great benefit among young people.
Keywords: Gingival overgrowth; Orthodontic therapy; Bacterial plaque; Oral hygene.
Citation: Rădeanu AC, Predescu AM, Stanca AG, Surpățeanu M, Andrei EC, et al. Implications of bacterial plaque in gingival overgrowth induced by orthodontic therapy. J Clin Images Med Case Rep. 2023; 4(9): 2581.
Introduction
Gingival overgrowth is a condition with increased incidence, especially in the case of children and adolescents [1]. In the case of children and adolescents, gingival overgrowth predominantly takes the following clinical forms: hereditary gingival fibromatosis [2], gingival overgrowth induced by type I neurofibromatosis [3], but also gingival overgrowth induced by the administration of drugs such as: nifedipine, phenytoin, cyclosporine A [1,4].
The increase in volume of the gingival tissue induced by drugs is a local lesion caused mainly by the side effects of drug therapy with phenytoin, nifedipine or ciclosporin. Nifedipine is a first-generation calcium channel blocker used for the treatment of hypertension and angina pectoris [5]. The onset of the lesion occurs at the level of the interdental papilla, with a tendency to extend until the entire dental crown is covered. The gingival mucosa in most cases maintains its pink color, has a firm consistency and does not show a tendency to bleed. In situations where gingival overgrowth takes on a severe, generalized form, it can affect dental occlusion [6].
Phenytoin was formerly known as diphenylhydantoin and is a potent anticonvulsant used to treat and prevent generalized seizures, complex partial seizures, and status epilepticus [7]. From the point of view of the clinical aspect, gingival overgrowth induced by phenytoin is characterized by slow growth that begins at the level of the interdental papilla, but which in the absence of inadequate hygiene or in the case of incorrect administration of the medication can lead to an excessive growth of the gingival mucosa reaching to cover the entire dental crown [7,8]. Also, in the case of Hg induced by phenytoin, a lesion with a high degree of fibrosis is observed [9].
Cyclosporin A is a selective and reversible immunosuppressive agent that is widely used as a drug for a wide spectrum of human diseases, such as graft-versus-host disease, noninfectious uveitis, rheumatoid arthritis, psoriasis, and atopic dermatitis [10]. Clinically, the gingival lesion induced by ciclosporin A is characterized by hyperemia, bleeding both during probing and brushing, or even spontaneous bleeding. The location of the lesion mainly affects the anterior area of the teeth [11].
Hereditary gingival fibromatosis is a rare condition, characterized by a slow progressive growth of the gingival mucosa, being the most common generalized form. The severity of gingival tissue growth causes phonetic and masticatory problems but can lead to diastemas or incorrect position of the teeth [12].
Recent studies have shown that gingival overgrowth can also be induced by orthodontic therapy [13]. Gingival overgrowth due to orthodontics has several possible causes: the accumulation of bacterial plaque and tartar caused by improper oral hygiene [13,14]; the material from which the orthodontic appliance is made [15]; overloading the periodontium by exercising excessive forces [16].
The material from which the orthodontic appliance is made is susceptible to the development of allergic reactions at the level of the gingival mucosa. Thus, we emphasize that over time a series of allergic manifestations induced by the orthodontic appliance have been reported due to the degree of corrosion of the material [17], the use of alloys with high allergenic potential: nickel-titanium [17], iron-nickel-chromium, cobalt-chromium [18]. Severe gingival overgrowth can lead to damage to aesthetic and masticatory functions, necessitating surgical excision of excess tissue [19].
Material and methods
Our study included a number of 15 subjects diagnosed with gingival overgrowth due to orthodontic reasons. The subjects presented themselves at the Oro-Maxillo-Facial Surgery Clinic in the city of Craiova, Romania, complaining of gingival bleeding, functional and masticatory disorders, but also of an aesthetic nature. Each subject was given a file, anamnesis, general and local clinical examination and were entered into a database created in the Excel program that includes information related to sex, age group, occupation, systemic diseases, allergies, drug treatments or surgical, O’Leary Plaque Index, duration of orthodontic treatment, age of the gingival overgrowth lesion. The informed consent of each subject was obtained.
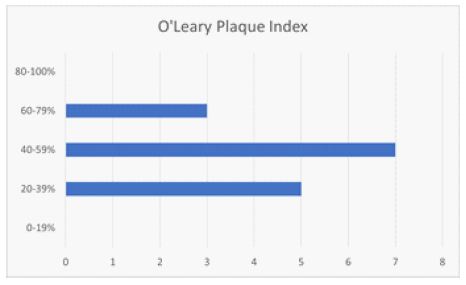
For each subject we calculated the O’Leary Plaque Index according to the formula:
PI = total number of surfaces with bacterial plaque/ total number of surfaces examined x100
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by Ethics Committee of the University of Medicine and Pharmacy Craiova (approval reference no. 39/01.03.2022).
Results
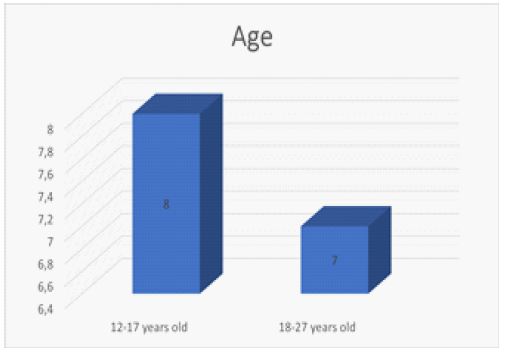
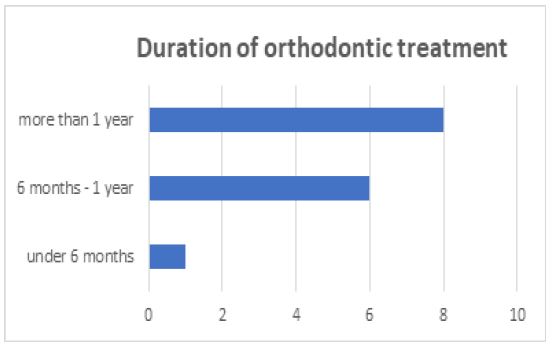
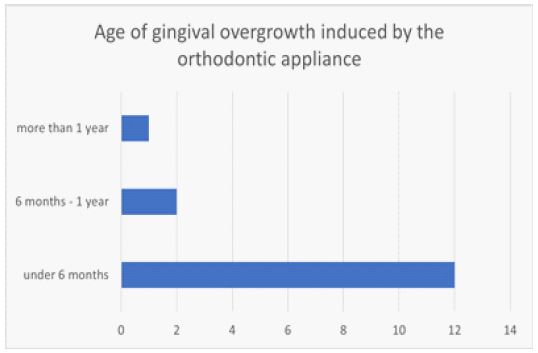
The subjects are included the age group of 12-27 years. Our study highlighted the fact that gingival overgrowth induced by orthodontic therapy tends to affect more male subjects (73.3%) than female subjects (26.6%). All subjects were tested for allergy to metal alloys from which the dental appliances are made, but no subject showed hypersensitivity. For each subject we calculated the O’Leary Plaque Index and it can be seen that most subjects had a score between 40-59%, this being a percentage worryingly, the duration of orthodontic treatment varies between 2 months and 3 years, most subjects are included the category of more than 1 year, and the age of gingival overgrowth varies between one month and 6 months. At the same time, it was noticed that subjects who have had orthodontic appliances for more than a year that the gingival overgrowth has a generalized form, being much more severe. Gingival lesions are detected in the early stages, often because the subjects go for regular check-ups once a month.



Discussion
Orthodontic therapy requires increased attention to maintaining oral hygiene. If the subject wearing orthodontic appliances does not strictly follow the rules of oral hygiene, the accumulation of bacterial plaque and tartar will occur, leading to the appearance of gingival inflammation. The severity of gingival inflammation depends on the amount of accumulated bacterial plaque [20,21]. In any situation, fixed orthodontic therapy leads to bacterial plaque retention, which requires the use of special tools and hygiene such as orthodontic mini-brushes that penetrate between the braces, the use of mouthwash or oral irrigator [21,22]. In the case of young subjects, we can use interactive methods of education regarding oral hygiene, such as the use of the bacterial plaque revealer [23].
For teenagers, the plaque revealing tablet method is not interesting, but we can use digital technology to capture attention [24]. An efficient method is represented by the installation of a smartphone application called WhiteTeeth app intended for patients with fixed orthodontic appliances [24]. This application can be easily used at home by the adolescent and has a motivational effect, an informative function on the negative effects on the teeth in case of non-compliance with hygiene rules throughout the wearing of the orthodontic appliance, a reminder function on the actions that must be performed [24].
Most orthodontists recommend that orthodontic therapy be initiated during adolescence, but they lose sight of the fact that this period is dominated by hormonal changes that favor the appearance of gingival inflammation [25]. Even in our study we observe the fact that all the subjects wearing dental braces are teenagers. We also noticed that most of the subjects of our study did not follow the instructions for maintaining oral hygiene recommended by the doctor, which led to the development of excessive gingival hypertrophies. Another problem, noted in our study, was represented by the use of excessive, incorrectly directed orthodontic forces that induced gingival overgrowth.
Conclusion
Bacterial plaque significantly influences the evolution and severity of gingival overgrowth induced by orthodontic therapy. The dentist has the duty to educate the patient and draw his attention to the fact that during orthodontic treatment the hygiene rules are much more rigorous, because braces are elements that retain bacterial plaque and food debris. Currently, there are many attractive techniques for familiarizing children and adolescents with the rules of oral hygiene that can be performed both at home and in the doctor’s office. Access to the applications aimed at this topic installed on the smartphone bring a great benefit among young people.
References
- Doufexi A, Mina M, Ioannidou E. Gingival Overgrowth in Children: Epidemiology, Pathogenesis, and Complications. A Literature Review. Journal of Periodontology. 2005; 76(1): 3–10.
- Dani N, Khanna DP, Vaibhavi Hitesh Bhatt, Joshi C. Idiopathic gingival fibromatosis. Journal of Indian Society of Periodontology [Internet]. 2015 [cited 2023 Aug 8]; 19(6): 698–8. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4753719/
- Thota E, John Jims Veeravalli, Sai Krishna Manchala, Bhargavi Priya Lakkepuram, Jayasurya Kodapaneni, Chen Y, et al. Age-dependent oral manifestations of neurofibromatosis type 1: a case–control study. Orphanet Journal of Rare Diseases [Internet]. 2022 [cited 2023 Aug 8]; 17(1). Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8889631/
- Zhang R, Wu J, Zhu J, Wang X, Song J. Bibliometric analysis of research trends and characteristics of drug-induced gingival overgrowth. Frontiers in Public Health. 2022; 10.
- Nifedipine [Internet]. PubMed. Bethesda (MD): National Institute of Diabetes and Digestive and Kidney Diseases; 2012. Available from: https://www.ncbi.nlm.nih.gov/books/NBK548324/
- Bajkovec L, Mrzljak A, Likic R, Alajbeg I. Drug-induced gingival overgrowth in cardiovascular patients. World Journal of Cardiology. 2021; 13(4): 68–75.
- Corrêa JD, Queiroz-Junior CM, Costa JE, Teixeira AL, Silva TA. Phenytoin-Induced Gingival Overgrowth: A Review of the Molecular, Immune, and Inflammatory Features. ISRN Dentistry [Internet]. 2011; 2011: 1–8. Available from: https://www.hindawi.com/journals/isrn/2011/497850/
- Seymour RA, Ellis JS, Thomason JM. Risk factors for drug-induced gingival overgrowth. Journal of Clinical Periodontology. 2000; 27(4): 217–23.
- Chacko LN, Abraham S. Phenytoin-induced gingival enlargement. BMJ Case Reports [Internet]. 2014 [cited 2020 Aug 7]; 2014. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4039754/
- Padjasek M, Qasem B, Cisło-Pakuluk A, Marycz K. Cyclosporine A Delivery Platform for Veterinary Ophthalmology—A New Concept for Advanced Ophthalmology. Biomolecules. 2022; 12(10): 1525.
- Ramalho VLC, Ramalho HJ, Cipullo JP, Burdmann EA. Hiperplasia gengival induzida por ciclosporina A. Revista da Associação Médica Brasileira. 2003; 49(2): 210–3.
- Strzelec K, Dziedzic A, Łazarz-Bartyzel K, Grabiec AM, Gutmajster E, Kaczmarzyk T, et al. Clinics and genetic background of hereditary gingival fibromatosis. Orphanet Journal of Rare Diseases. 2021; 16(1).
- Rathod AD, Jaiswal P. Gingival overgrowth during orthodontic treatment and its management. Pan African Medical Journal. 2022; 42.
- Gaur S, Agnihotri R. Is dental plaque the only etiological factor in Amlodipine induced gingival overgrowth? A systematic review of evidence. Journal of Clinical and Experimental Dentistry. 2018.
- Orozco-Páez J, Méndez-Rodríguez MA, Rodríguez-Cavallo E, Díaz-Caballero A, Méndez-Cuadro D. Protein carbonylation associated with nickel liberation in orthodontic gingival overgrowth. Archives of Oral Biology. 2021; 125: 105103.
- Surlin P, Rauten AM, Mogoantă L, Siloşi I, Oprea B, Pirici D. Correlations between the gingival crevicular fluid MMP8 levels and gingival overgrowth in patients with fixed orthodontic devices. Romanian Journal of Morphology and Embryology = Revue Roumaine De Morphologie Et Embryologie [Internet]. 2010 [cited 2023 Aug 8]; 51(3): 515–9. Available from: https://pubmed.ncbi.nlm.nih.gov/20809029/
- Espinoza-Montero PJ, Montero-Jiménez M, Fernández L, Paz JL, Piñeiros JL, Ceballos SM. In vitro wearing away of orthodontic brackets and wires in different conditions: A review. Heliyon. 2022; 8(9): e10560.
- Schiff N. Galvanic corrosion between orthodontic wires and brackets in fluoride mouthwashes. The European Journal of Orthodontics. 2005; 28(3): 298–304.
- Ballini A, Scattarella A, Crincoli V, Carlaio RG, Papa F, Perillo L, et al. Surgical treatment of gingival overgrowth with 10 years of follow-up. Head & Face Medicine. 2010; 12: 6(1).
- Pellegrini P, Sauerwein R, Finlayson T, McLeod J, Covell DA, Maier T, et al. Plaque retention by self-ligating vs elastomeric orthodontic brackets: quantitative comparison of oral bacteria and detection with adenosine triphosphate-driven bioluminescence. American Journal of Orthodontics and Dentofacial Orthopedics: Official Publication of the American Association of Orthodontists, Its Constituent Societies, and the American Board of Orthodontics [Internet]. 2009 [cited 2022 Apr 10]; 135(4): 426.e1-9; discussion 426-427. Available from: https://pubmed.ncbi.nlm.nih.gov/19361723/
- Vincent-Bugnas S, Borsa L, Gruss A, Lupi L. Prioritization of predisposing factors of gingival hyperplasia during orthodontic treatment: the role of amount of biofilm. BMC Oral Health. 2021; 21(1).
- Ren X, Zhang Y, Xiang Y, Hu T, Cheng R, Cai H. The efficacy of mouthwashes on oral microorganisms and gingivitis in patients undergoing orthodontic treatment: a systematic review and meta-analysis. 2023; 23(1).
- Fasoulas A, Pavlidou E, Petridis D, Mantzorou M, Seroglou K, Giaginis C. Detection of dental plaque with disclosing agents in the context of preventive oral hygiene training programs. Heliyon. 2019; 5(7): e02064.
- Scheerman JFM, van Meijel B, van Empelen P, Kramer GJC, Verrips GHW, Pakpour AH, et al. Study protocol of a randomized controlled trial to test the effect of a smartphone application on oral-health behavior and oral hygiene in adolescents with fixed orthodontic appliances. BMC Oral Health. 2018; 18(1).
- Studen-Pavlovich D, Ranalli DN. Periodontal and Soft Tissue Prevention Strategies for the Adolescent Dental Patient. Dental Clinics of North America. 2006; 50(1): 51–67.