
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Efficacy of platelet-rich plasma treatment in a young athlete with osgood-schlatter disease and patellar tendinopathy, suffering from familiar mediterranean fever: A case report
Angelo Paolo Amico1*; Maria Vittoria Raele1; Maria Cusmai1; Claudia Citarella2; Marisa Megna1; Maurizio Ranieri1
1Department of Translational Biomedicine and Neuroscience (DiBraiN), Aldo Moro University, 70121 Bari, Italy.
2Department of Transfusional Medicine, Aldo Moro University, 70121 Bari, Italy.
*Corresponding Author : Angelo Paolo Amico
Department of Translational Biomedicine and Neuroscience (DiBraiN), Aldo Moro University, 70121 Bari, Italy.
Tel: +39 0805595416;
Email: paolo-amico@alice.it
Received : Aug 08, 2023
Accepted : Sep 01, 2023
Published : Sep 08, 2023
Archived : www.jcimcr.org
Copyright : © Amico AP (2023).
Abstract
Background: Osgood-Schlatter Disease (OSD) is one of the most common causes of anterior knee pain in children and adolescents. It is a condition with a tendency to self-resolve, and as a result, treatment is symptomatic. In the few resistant and persistent cases, surgical treatment is opted for. Familial Mediterranean Fever (FMF) is a condition due to a genetic mutation that predisposes to the risk of complicated enthesitis. Platelet-Rich Plasma (PRP) is a type of regenerative medicine based on the injection of autologous growth factors capable of regenerating injured tissues.
Methods: A 14-years old patient with FMF, left-dominant OSD and a left therapy resistant patellar tendon enthesitis was recruited. Knee pain and function were assessed with Visual Analogic Scale (VAS), Western Ontario and McMaster University (WOMAC) and knee ultrasound evaluation. The patient was evaluated at T0, at the end of the PRP Treatment (T1) and two months after the end of the Treatment (T2). Moreover, a knee MRI was collected at T0 and T2.
Results: At T1 and still at T2, the VAS and WOMAC scales showed a statistically significant decrease compared with the mean value at T0 and the sonographic images showed a complete resolution of the signs of disease.
Conclusion: PRP has showed to be an effective and safe method in OSD treatment in a 14-years-old athlete with a concomitant patellar tendon enthesitis and FMF. The treatment enabled the 14-year-old athlete to return to competitive basketball and avoid surgery, completely resolving his symptoms.
Keywords: Osgood-schlatter; Familial mediterranean fever; Platelet-rich plasma; Regenerative medicine; Patellar tendon enthesitis.
Citation: Amico AP, Raele MV, Cusmai M, Citarella C, Megna M, et al. Efficacy of platelet-rich plasma treatment in a young athlete with osgood-schlatter disease and patellar tendinopathy, suffering from familiar mediterranean fever: A case report. J Clin Images Med Case Rep. 2023; 4(9): 2583.
Introduction
Osgood-Schlatter Disease (OSD) is one of the most common causes of anterior knee pain in children and adolescents [1]. It is a distinctly juvenile medical condition, the onset of which is contributed by bone immaturity of the tibial tuberosity and an abnormal mechanism of traction of the patellar tendon against the tibial tuberosity itself [2]. It is caused by repeated contractions of the quadriceps muscle at the insertion of the proximal tibial apophysis often leading to small avulsion fractures [3]. To date, treatment involves interruption of competitive physical activity, use of analgesics, and physiotherapy [4]. However, the pain symptoms can persist for a long time, leading to surgery, with all the associated consequences and possible complications and psychological issues in affected patients [5].
Platelet-Rich Plasma (PRP) is a growing therapeutic option in musculoskeletal medicine [6]. It consists in a procedure that involves extracting blood directly from the patient to obtain an autologous plasma preparation enriched in platelets compared to physiologic concentrations [7]. The rationale of the treatment is based on the therapeutic role of a high platelet concentration in providing a supraphysiological amount of growth factors to provide the regenerative stimulus to tissues [8]. The aim of our case report is to assess the efficacy of PRP treatment in a surgery candidate 14-year-old patient with OSD and Familial Mediterranean Fever (FMF).
Case presentation
On October 2022, a 14-years-old male basketball player with a childhood history of OSD and FMF came to the Physical Medi-cine and Rehabilitation Unit of the Bari General Hospital, Italy, presenting a bilateral knee (left-dominant) pain since about 2 months. He denied direct impacts. On the MRI that the patient brought in for viewing (Oct 7th) there was: Evidence of severe OSD; inhomogeneous, thickened and edematous patellar tendon at distal preinsertion site; fragmented appearance of anterior tibial apophysis, with presence of subcortical intraspongious bone edema; fluid portion in anterior tibial recess where edematous imbibition of adjacent adipose tissue was appreciated; minimal retrorotular joint effusion, with reactive synovitis at the central pivot. At a previous orthopedic specialist visit, the patient was candidate for surgery.
At the first examination (T0), the last PRP treatment session (T1) and two months after the end of the treatment (T2), the patient underwent: Medical examination, ultrasound evaluation and rating scales to quantify pain and the impact of his condition on lifestyle. Specifically, the rating scales were:
• Visual Analogic Scale (VAS), one of the pain rating scales used to measure intensity or frequency of various symptoms. It goes from 0, no pain, to 10, the worst pain ever experienced (Figure 1).
• Western Ontario and McMaster University (WOMAC), a scale used in the evaluation of Hip and Knee Osteoarthritis. It consists of 24 items divided into 3 subscales: pain (5 items), stiffness (2 items) and physical function (17 items) (Figure 2).
On the first examination (October 31st) (T0), the informed consent was obtained from the mother and the patient himself.

At the medical examination he showed tenderness at the tibial tuberosity, but no overlying erythema or limited Range Of Motion (ROM).
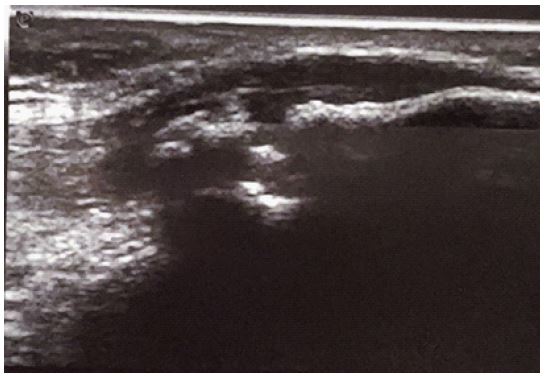
Sonographic imaging revealed irregularity of the tibial bone profile, presence of numerous diffuse calcifications and hypoechogenic thickening at the distal insertion of the patellar tendon (Figure 3).
It goes from 0, absence of disability from osteoarthritis, to 95, severe disability from osteoarthritis.
The score of rating scales were respectively: 8/10 (VAS) and 60/95 (WOMAC).
On this occasion, absolute functional rest was recommended to the patient with a methylsulfonylmethane cartilage supplement to be taken once per day for 2 months, an acetyl ester ointment to be applied twice per day for 20 days and an oral anti-edema to be taken once per day for 2 months. We scheduled the checkup after about two weeks.
On the second examination (November 16th), the patient had no benefits. The objective examination, ultrasound and subjective assessment using the scales had remained unchanged.
At this point, based on the existing literature on treatment of unresponsive OSD, we chose for PRP use.
Therefore, on the third examination (November 29th), we obtained 180 ml of venous blood directly from the patients. The blood samples were brought to the Transfusion Center of Bari General Hospital. Three aliquots of standardized PRP were obtained using a dedicated cell separator processing 60 ml of blood at a time. Each PRP aliquot had a platelet concentration 18 times higher than the patient’s baseline platelet values.
With ultrasound guidance, one of the three autologous plasma sample was injected at the level of the insertion of the patellar tendon of the left knee, which was found to be the most damaged.
We suggested cryotherapy and functional rest at home.
The remaining PRP tubes were stored at the blood bank of the Bari General Hospital at a temperature of -40°C until two hours before the second and the third injections and injected at the same site and always by the same doctor under ultrasound guidance, weekly, for a total of 3 administrations and specifically on December 7th and 13th (T1).
At the last treatment session (T1), the medical examination showed a reduction in finger-press pain and an improvement in joint function.
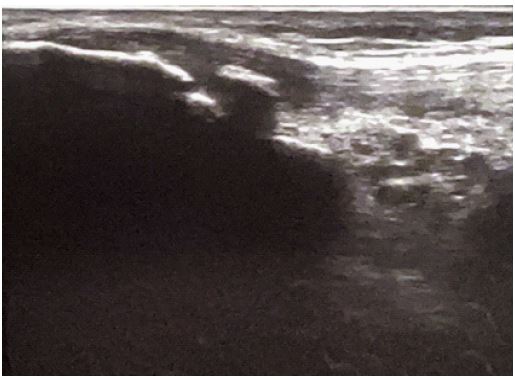
Sonographic imaging showed delimitation of the edematous area and ossification of the apophyseal nucleus (Figure 4).
In the same occasion, the patient was again subjected to the rating scales examined at T0 with the following results: 5/10 (VAS), 45/90 (WOMAC).
During treatment, the patient was instructed to manage any pain only with Paracetamol 1 gr (maximum 3 per day, at a time dis-tance of at least 8 hours) and cryotherapy and to record the relevant intakes in a proper diary.
Exactly two months after the end of the PRP treatment, and precisely on February 21st 2023, the patient returned for a follow-up visit (T2).
At the medical examination, the joint was completely pain-free.

Sonographic imaging revealed the complete resolution of tendon edema and fusion of the apophyseal rostrum with the rest of the apophysis (Figure 5).
Moreover, the rating scales had a significant improvement in subjective pain and quality of life: 0/10 (VAS), 5/90 (WOMAC).
In order to have a more objective and precise data, the patient underwent a new MRI which showed only an end result of the apophysitis, with a small bone protrusion of the tibial apophysis without the previous fragmentation of bone nuclei and without concomitant synovitis and tendonitis.
The patients had no side effects and he was able to re-start playing basketball.
Discussion
Apophysitis of the tibial tubercle, commonly known as OSD, is a self-limiting condition [9]. In fact, as the bone matures, this condition tends to resolve spontaneously in most cases [10]. Only for limited cases, when pain and consequently functional limitation persist into adulthood, it is possible to intervene with open surgery or arthroscopy, usually preferred because of the lower risk of postoperative complications [11]. Although treatment, in most cases, is only symptomatic, it is possible, as in our case, that the pain is very disabling [12]. Moreover, our patient was affected by FMF. Specifically, FMF is an autosomal recessive autoinflammatory disease due to a genetic mutation on the MEFV gene located on the short arm of chromosome 16 [13]. The diagnosis is mainly clinical as affected patients have frequent episodes of fever and serositis. The most fearsome complication is amyloidosis. The only effective treatment for this category of patients turns out to be colchicine, which has been used for about 40 years [14]. To date, it is known that this condition predisposes to an increased risk of developing exertional leg pain and enthesitis, that may slightly improve with underlying condition treatment, which is colchicine, but are more problematic and less easily responsive to common treatments [15]. Indeed, as demonstrated by the first MRI and ultrasound examination, our patient had severe apophysitis, synovitis and concomitant severe patellar tendon enthesitis, so he was candidate for surgery with all the possible complications and hospitalization time it would bring. This could prove to be a problem for young athletes, who are forced to stay away from their sports activities for a long time. In a study of Wolanin A. et al., it was well documented that having to give up sports because of health problems, can lead young athletes to social isolation and significant psychological issues [16]. For this reason, with a 14-year-old boy who was a basketball player at competitive levels, we tried to find an alternative that could somehow reintegrate him into sports.
The clinical use of PRP is based on the increase of growth factors concentration and in the secretion of proteins which are able to maximize the healing process at the cellular level [17]. Since PRP is an autologous biologic material, it involves a minimum risk of immune reactions and transmission of infectious and contagious diseases, and it has been widely used for the recovery of musculoskeletal lesions [18]. Despite the great potential for applicability, the implementation of the therapeutic use of PRP as a clinical alternative is poorly standardized, due to the lack of studies related to the standardization of the techniques and/or insufficient description of the adopted procedures [19]. Anyway, based on a previous 2021 systematic review which dealt with the long-term safety of certain types of treatment for osteoarthritis, we opted for 3 injections of PRP [20]. Moreover, a 2017 study by Danneberg Dirk-Jonas showed the efficacy of autologous conditioned-plasma infiltration in two OSD patients and specifically a 23-year-old male tennis player and a 14-year-old male patient which resulted pain-free after 3 weeks and 6 weeks respectively [21].
Our patient was treated with PRP for OSD and resistant patellar tendinopathy. In consideration of MRI imaging findings, our hypothesis was that treatment with PRP may have boosted the process of bone maturation in tibial apophysis, resolving the inflammation. These findings pair with the absence of pain and the total recover of all functions, which allowed the patient to go back to agonistic basketball practice [22]. Our goal was to seek a non-surgical treatment that could reduce pain and inflammation of the anterior knee, allowing return to sport and making so our patient’s lifestyle as similar as possible to that of his peers, in order to avoid psychological problems too; all of this safely, respect to FMF.
The main limitation of this study is the short duration of the follow-up and the small sample. For this reason, further studies are needed to monitor pain and joint function over time. Finally, there was not a placebo group, but this choice was due to the fact that he was the only patient with FMF and OSD and, anyway, it is necessary to guarantee a treatment for all patients suffering from a significant knee pain. Nevertheless, future studies will overcome this limitation, in compliance with the necessary ethical rules.
Conclusion
Even if OSD is a self-releasing disease, PRP has showed to be an effective and safe method in its treatment in a 14-years-old athlete with a concomitant patellar tendon enthesitis and FMF. It can therefore be used in selected very disabling cases, also in order to avoid surgery. New studies and more cases are needed to verify the follow-up and determine its efficacy over time.
Declarations
Funding: This research received no external funding.
Institutional review board statement: Not applicable.
Informed consent statement: Informed consent was obtained from all subjects involved in the study.
Data availability statement: The datasets used and analyzed during the current study will be made available upon reasonable request to the corresponding author, A.P.A.
Acknowledgments: None.
Conflicts of interest: The authors declare no conflict of interest.
Disclaimer/publisher’s note: The statements, opinions and data contained in all publications are solely those of the individual author (s) and contributor (s). The journal/editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content.
References
- Gholve PA, Scher DM, Khakharia S, Widmann RF, Green DW. Osgood Schlatter syndrome. Curr Opin Pediatr. 2007; 19: 44-50.
- Lucenti L, Sapienza M, Caldaci A, Cristo C, Testa G, et al. The Etiology and Risk Factors of Osgood-Schlatter Disease: A Systematic Review. Children (Basel). 2022; 9: 826.
- Ladenhauf HN, Seitlinger G, Green DW. Osgood-Schlatter disease: A 2020 update of a common knee condition in children. Curr Opin Pediatr. 2020; 32: 107-112.
- Neuhaus C, Appenzeller-Herzog C, Faude O. A systematic review on conservative treatment options for OSGOOD-Schlatter disease. Phys Ther Sport. 2021; 49, 178-187.
- Shamov, I.A. [OSGOOD-SCHLATTER DISEASE]. Klin Med (Mosk). 2016; 94: 144-8.
- Wu, P.I, Diaz, R, Borg-Stein, J. Platelet-Rich Plasma. Phys Med Rehabil Clin N Am. 2016; 27: 825-853.
- Martínez-Martínez A, Ruiz-Santiago F, García-Espinosa J. Platelet-rich plasma: Myth or reality? Radiologia. 2018; 60: 465-475.
- Southworth TM, Naveen NB, Tauro TM, Leong NL, Cole BJ. The Use of Platelet-Rich Plasma in Symptomatic Knee Osteo-arthritis. J Knee Surg. 2019; 32: 37-45.
- Dunn JF. Osgood-Schlatter disease. Am Fam Physician. 1990; 41: 173-6.
- Bezuglov EN, Tikhonova АА, Chubarovskiy PV, Repetyuk АD, Khaitin VY, et al. Conservative treatment of Os-good-Schlatter disease among young professional soccer players. Int Orthop. 2020; 44: 1737-1743.
- Mun F, Hennrikus, WL. Surgical Treatment Outcomes of Unresolved Osgood-Schlatter Disease in Adolescent Athletes. Case Rep Orthop. 2021; 2021: 6677333.
- Vaishya R, Azizi AT, Agarwal AK, Vijay V. Apophysitis of the Tibial Tuberosity (Osgood-Schlatter Disease): A Review. Cu-reus. 2016; 8: e780.
- Kucuk A, Gezer IA, Ucar R, Karahan AY. Familial Mediterranean Fever. Acta Medica (Hradec Kralove). 2014; 57: 97-104.
- Buades Reinés J, Aguirre Errasti C. Fiebre mediterránea familiar [Familial Mediterranean fever]. Med Clin (Barc). 2001; 117: 142-6.
- Tezcan ME, Volkan O, Mercan R, Sen N, Yilmaz-Oner S. Familial mediterranean fever patients may have unmet needs for the treatments of exertional leg pain and enthesitis. Reumatol Clin. 2022; 18: 227-230.
- Wolanin A, Gross M, Hong E. Depression in athletes: Prevalence and risk factors. Curr Sports Med Rep. 2015; 14: 56-60.
- Everts P, Onishi K, Jayaram P, Lana JF, Mautner K. Platelet-Rich Plasma: New Performance Understandings and Therapeu-tic Considerations in 2020. Int J Mol Sci. 2020; 21: 7794.
- Sheean AJ, Anz AW, Bradley JP. Platelet-Rich Plasma: Fundamentals and Clinical Applications. Arthroscopy. 2021; 37: 2732-2734.
- Marques LF, Stessuk T, Camargo IC, Sabeh Junior N, dos Santos L, et al. Platelet-rich plasma (PRP): Methodological as-pects and clinical applications. Platelets. 2015; 26: 101-13.
- Charlesworth J, Fitzpatrick J, Perera NKP, Orchard J. Osteoarthritis- a systematic review of long-term safety implications for osteoarthritis of the knee. BMC Musculoskelet Disord. 2019; 20: 151.
- Danneberg DJ. Successful Treatment of Osgood-Schlatter Disease with Autologous-Conditioned Plasma in Two Patients. Joints. 2017; 5: 191-194.
- Grassi A, Napoli F, Romandini I, Samuelsson K, Zaffagnini S, et al. Is Platelet-Rich Plasma (PRP) Effective in the Treatment of Acute Muscle Injuries? A Systematic Review and Meta-Analysis. Sports Med. 2018; 48: 971-989.