
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Research Article - Open Access, Volume 4
Alzheimer’s disease and caregiver’s burden: The efficacy of a psychoeducational and psychotherapeutic groups
Letteria Tomasello1,2*; Claudio Zaccone1; Santi Galletta3; Angelina Laganà4; Claudia Pitrone3; Massimo Raffaelev1; Amelia Brigandì5; Angela Alibrandi6
1Department of Clinical and Experimental Medicine, University of Messina, 98122 Messina, Italy.
2Faculty of Medicine and Dentistry, Sapienza University of Rome, 00185 Rome, Italy.
3Réseau Hospitalier Neuchâtelois (RHNe), Service de Neurologie et Neuroréadaptation, 2000 Neuchâtel, Switzerland.
4Department of Biomedical and Dental Sciences, Morphological and Functional Images, 98122 Messina, Italy.
5IRCCS Neurolesi “Bonino Pulejo”, Messina, Italy.
6Departiment of Ecomomics, University of Messina, Italy.
*Corresponding Author : Letteria Tomasello
Department of Clinical and Experimental Medicine, University of Messina, 98122 Messina, Italy.
Email: ltomasello@unime.it
Received : Aug 08, 2023
Accepted : Sep 04, 2023
Published : Sep 11, 2023
Archived : www.jcimcr.org
Copyright : © Tomasello L (2023).
Abstract
Alzheimer’s Disease (AD) accounts for 54% of cases of dementia. The risk of Alzheimer increases with age and women seem to be more easily affected. Age is considered the most important risk factor for the disease. Cognitive impairment is the most evident symptom. Dementia is now considered a “social disease” because it involves not only the patient involved, but also the social network in which he/she lives. Existing welfare practices do not totally fulfil the needs of people with dementia and 80% of caregivers choose to treat family members at home, even if it is detrimental of their health and quality of life. Such disorders are highly influenced (and often activated) by environmental factors, especially by the relationship between patients and their caregivers. Nowadays, health care relies on patient’s relatives with severe and various repercussions on those assisting, such as fatigue, psychological pain, mental disorders, physical illnesses. The bio-medical approach is based on the pathology and on interventions aimed to mitigate the symptoms or to cure the disease. For this reason, it’s worthy to reaching the improvement of the quality of life, rather than focusing simply on health care. This paper describes the care burden and the efficiency of psycho-educational groups associated with psychotherapy according to the bio-psychosocial model.
Citation: Tomasello L, Zaccone C, Galletta S, Laganà A, Pitrone C, et al. Alzheimer’s disease and caregiver’s burden: The efficacy of a psychoeducational and psychotherapeutic groups. J Clin Images Med Case Rep. 2023; 4(9): 2585.
Introduction
Dementia is a chronic pathological neurodegenerative process leading to progressive decline in cognitive and functional abilities [1,2]. According to the World Health Organization (WHO, 2015), the number of people living with dementia diagnoses in 2015 was approximately 47 million people in the world. This number is projected to increase to approximately 76.36 million people worldwide in 2030 a 60.86% increase and up to 131 million people worldwide in 2050. This increase in prevalence rates is likely due to the growing population and increasing life expectancy of the general population. The projected increase in dementia prevalence rates constitutes a serious issue around the world. The prevalence rates of specific types of dementia disorders vary throughout the literature due to a lack of methodological uniformity and consistency in diagnostic criteria used across studies [3,4]. Alzheimer’s Disease (AD) comprises most of all dementia diagnoses, with 60-80% of all dementia diagnoses being that of the AD type [5], in particular, age is considered the most important risk factor for the disease, the prevalence doubles in every five-year increment in age after 65 years of age and it is one of the major causes of disability in later life [6]. Most importantly, this is not an inevitable or normal part of ageing, cognitive impairment is the most evident symptom and includes memory and time impairment, spatial disorientation, and behavioural issues. The disease affects different cognitive functions and does not involve all individuals equally [1,2]. Moreover, it provokes a radical change in the people affected: Things that were simple to do in the past become hard to achieve. Patients are not able to manage the external inputs and become confused. Confusion generates discomfort and produces a negative emotional response. Dementia is now considered a “social disease” because it involves the whole family nucleus of the patient. Furthermore, deficits occur in every individual with different levels of clinical severity and the reaction to these losses will be individual, so as to determine a radical change in the person and a difficulty in doing things compared to the past, with possible modification of the temper [7].
In dementia, the mental capacity to control stimuli decreases, confusion expands, and the patient feels frightened, vulnerable, out of control, no longer able to control and manage emotions and with difficulty in interpreting the surrounding events and in relating to them in reasonable way. The disease causes a progressive decline of the individual as a “person” because it progressively disintegrates what has been, who he/she is now and who he/she will be, what he/she can do, how he/she can move around the world. Therefore, the things he/she thought and did in the past will become impossible goals to achieve [8].
The majority of patients with dementia experience “Behaviour And Psychological Symptoms Of Dementia” (BPSD) at some point: when community dwelling individuals with dementia have undergone assessment in longitudinal studies, up to 97% are affected [9] neuropsychiatric disorders include impairments in motivation, interest, social behaviour and awareness, mood disorders, anxiety, agitation, impulsivity, and hallucinations and delusions, all of which often require clinical intervention. Among psychotic symptoms, hallucinations and delusions are the most clinically relevant, and are associated with hospitalization or institutionalization, cognitive and functional impairment, accelerated cognitive decline and mortality, as well as caregiver distress [10,11] on cognitive symptoms as behavioural and psychological symptoms of dementia are distressing for people with AD but also for their caregivers, with poor outcomes in terms of function, quality of life, disease course, mortality, and economic cost [12,13]. The biopsychosocial approach has proposed that neuropsychiatric disturbances which usually appear earlier than the cognitive symptoms, are the effects of the interactions between an individual’s biology, prior experiences, and current environment. Dementia related agitation, disinhibition, and psychosis are associated with volume reductions and decreased metabolism in the orbital and dorsolateral prefrontal cortex, anterior cingulate, insula, and temporal lobes-parts of the brain that mediate emotional regulation, self-awareness, and perception; and apathy is associated with small vessel white matter disease [14] Moreover, BPSD are highly influenced (and often activated) by environmental factors, especially by the relationship between the patient and the caregivers.
Caregiver is a word defining those people who look after or help someone who is sick. Becoming a caregiver often means to take on a role for some people that are not prepared and instructed. To become a caregiver means to be able to take care in its deep meaning; then, it requires an adequate training. Nowadays, health care relies on patient’s relatives with severe and various repercussions on those assisting. The negative impact of caring for a person with dementia is often conceptualized in terms of caregiver burden [15]. Caregiver burden and its risk factors have been investigated in numerous studies, putting in light some burden-related concepts such as fatigue, psychological pain, mental disorders, physical illnesses. The behavioural problems and mood disorders of patients were consistently reported as important risk factors for caregiver burden. Neuropsychiatric disturbances usually appear earlier than the cognitive symptoms as a result of the heterogeneous neuropathic and neurochemical alterations present in different kinds of dementia. The prevalence of BPSD in people with dementia is estimated to be as high as 97% [16,17]. Families are deeply involved in the process of care and homecare and are faced with enormous physical and psychological stresses linked to the disease and the changes it determines in the person affected. Existing welfare practices do not meet the needs of people with dementia and 80% of caregivers choose to treat family members at home, often to the detriment of their health and quality of life [18]. The social networks and society can be compromised, and people living with dementia become increasingly dependent on their caregivers. Families are deeply involved in the process of care and homecare, typically their spouses or children. Informal caregivers play an important role for people with dementia, helping them in their daily activities, whose dependence increases with severity of the disease [19]. It is known that the progression of the disease leads to greater confusion and less control over behaviour in the patient, and therefore has a profound meaning, as a reaction or response to needs, impulses, emotions, desires [20]. The bio-medical approach is based on the pathology and on interventions aimed to mitigate the symptoms or to cure the disease. For this reason, it’s worthy to have as a goal the improvement of the quality of life, rather than focusing simply on health care. A systematic review of Chiao et al. 2015 reported patients’ functional status, behavioural problems, and levels of neuropsychiatric symptoms as most burdensome to informal caregivers. The consequence is that people living with dementia may feel lonely or isolate or are not engaging in meaningful activities with decreased quality of life [21-23]. Some examples of relationship problems are the following: “My future plans and hopes vanished from I have to take care of this sick person”; “I had to leave my job and give up my hobbies in order to take care of him”; “He is not the same sweet person I married; he can’t recognize me”; “I can’t go out because no one can help me; he gets mad at everybody except me”.
Materials and methods
Clinical objectives: The clinical objectives were to provide to the caregivers the right emotional support, in order to relieve them from their burden; to limit social isolation through the possibility to share the experience; to develop the necessary skills to analyse the self-directed relational patterns; to show alternative behavioural modalities.
Objective: The objective of our study was to evaluate the care burden and the efficiency of psycho-educational groups associated with psychotherapy according to the bio-psychosocial model.
Specific objectives: Specific objectives were to reduce caregiver’s needs and also indirectly the caregiver burden and depression; to learn management skills to carry out the role; to start an inner path in order to reach a self-awareness and to disclose eventual difficult familiar relationships. The Group integrated therapeutic groups and psychological support setting with that one of the groups defined as “training”. The intervention was focused on two levels: (i) to reach knowledge about the disease and the strategies to deal with it; (ii) to highlight psychological needs of group’s participants (sharing of the caregiver experience), to allow emotional elaboration related to the experience itself and to the experience considering the familiar link.
Caregiver patients: We enrolled 25 informal main caregivers (19 women and 6 men) of patients with probable AD, mild to moderate. In order to monitor the needs of the family, it was decided not to include professional assistance figures in this research. All informed caregivers were submitted to Caregiver Burden Inventory (CBI), Hamilton Depression Rating Scale (HAM-D), Activity of Daily Living (ADL), Instrumental Activity of Daily Living (IADL), both before participating in the study and at the end. All subjects completed the study. We also enrolled 25 patients (21 females 4 males) with a Mini Mental State Examination (MMSE) of >15 and probable AD according to the NINCDS-ADRDA criteria (McKhann, G., et al. 1984) [24], who consecutively attended the Memory Clinic of our Department in Messina. The mean age was 75.7 years and the mean MMSE score was 19.23. The cognitive levels were investigated by MMSE, MODA, Activity Daily Living, and IADL. The diagnosis of dementia syndromes was based on clinical, neuropsychological, laboratory, and neuroimaging data according to current research criteria. Patients with severe neuro-sensory deficits, psychiatric diseases, and alcohol/substance abuse were excluded. Before being interviewed, all participants gave the informed consent to participate in this study. They were assured that the transcript of the interview would remain strictly confidential and that patients would not be named in the final description and analysis.
Instrumental evaluation: CBI [25] is a rapidly compiling scale that measures the care burden created for caregivers of patients with AD and related dementias. It is a self-report tool, which must be completed by the main caregiver. It is structured according to a multidimensional perspective. The CBI is divided into 5 sections that measure the different aspects of the care burden: objective, psychological, physical, social, and emotional. The burden depending on the time required for assistance (T) (items 1-5) describes the load associated with the restriction of time for the caregiver. The evolutionary burden (S) (item 6-10) is the isolation perception of the caregiver, also considering the expectations and opportunities of their peers. The physical burden (F) (item 11-14) describes the feeling of chronic fatigue and somatic health problems while the social burden (D) examines the perception of a role’s conflict. The emotional burden (E) (items 20-24) describes the feelings towards the patient, which can be induced by behavioural disorders of the latter. Each section consists of 5 items and the score for each individual item goes from 0 (factor with minimum value) to 4 (factor with maximum value), for a total ranging from 0 to 20 for each dimension, except for the physical burden which is composed of 4 items. A correction factor of 1.25 is then applied to the total score. The range of the total score varies from 0 to 100. The scores for each section increase proportionally to the perceived severity of the burden for each area; therefore, with the same total score, the burden profiles may be very different. These so defined profiles will be the evaluation basis on which to build ad-hoc psycho- social interventions.
HAM-D [26] investigates different areas for assessing the depressive state of a subject. It cannot be used as a diagnostic tool for depression, but it allows to quantitatively assess the severity of the subject’s conditions and to document the modifications of these conditions, for example during a psychotherapeutic treatment. The HAM-D consists of 21 items. The severity cut-off is ≥25 severe depression, 18-24 moderate depression, 8-17 mild depression, ≤7 absence of depression.
Clinical Dementia Rating (CDR) scale [27]. The necessary information was collected through a family member or operator who knows the subject and through an assessment of the patient’s cognitive functions. Each aspect must be evaluated independently from the others. Memory is considered a primary category; the others are secondary. If at least three secondary categories get the same of memory score, then the CDR is equal to the score obtained in the memory. If three or more secondary categories obtain a higher or lower value of the memory, then the CDR score corresponds to that obtained in most secondary categories. If two categories obtain a higher value and two a lower value than that obtained from the memory, the CDR value corresponds to that of the memory. The scale was later extended to classify the more advanced stages of dementia with better precision (Hayman et al. 1987). Patients can therefore be classified in stage 4 (very severe dementia) and stage 5 (terminal dementia) when they require total assistance because they are completely incapable of communicating, in a vegetative state, bedridden or incontinent.
The MMSE [28] is used as a screening test in the assessment of the general cognitive state. It is a quick administration tool consisting of 11 items; it explores capabilities such as space-time orientation, fixation memory, attention and calculation, immediate and delayed re-enactment of verbal material, language, constructive praxis. The maximum score is 30; scores equal to or greater than 24 are considered to be within normal limits; slight deficit between 21 and 23, average between 11 and 20, severe between 0 and 10; the raw score is corrected based on age and education.
Psychoeducational group: The intervention was done in seven meetings. In each meeting caregivers were compared with a specific theme which was considered important for the management of patients affected by this pathology (neuropsychological and behavioural aspects of dementia). Each meeting lasts 1 hour and 30 minutes, it was settled weekly, and the number of participants was variable, minimum 8 and maximum 13.
Meeting layout: Introduction and explanation of the meeting’s theme: every theme was defined in a simple but correct way, reducing the use of scientific terms. The definition of the theme was very important because it allowed us to work on the specific symptoms of the patients and on the respective “answer” of the caregiver. The conduction was entrusted to a Psychologist/Psychotherapist, with training in Neuropsychology, and there was also a participant observer (specialist in Neurology and an external observer).
Meeting program: First meeting: Introduction to disease and intervention, memory disorders and language disorders, attention, and space-time orientation Second meeting: Development of daily life activities and personal care. Third meeting: Depression, apathy, irritability, and anxiety. Fourth meeting: Aggressiveness, restlessness (agitation) and disorders of psychomotor activity. Fifth meeting: Disinhibition, delusions, and hallucinations. Sixth meeting: Neurovegetative alterations. Seventh meeting: Reflections on the welfare of the caregiver (burn-out). Sharing/confronting moment among caregivers: Every caregiver expressed the real symptoms according to the discussed theme and to the daily situations that are more stressful and harder to handle. Analysis of the strategies and of the behavioural, communicative, and emotional ways used by the caregiver in order to cope with these situations and confutation of the eventual wrong interpretations towards patients. Distinction of the effective strategies and of ineffective and unadaptable strategies. Suggestion of new relation ways and of more effective solutions for coping the situation. The aim of the psychoeducational group was to act on thoughts and emotions connected to the problematic situation in order to modify the answers. The typology of intervention was based on two levels: (i) practical objectives (to have practical knowledge of the pathology and know what to do for coping with it); (ii) psychological needs of the participants of the group (sharing caregivers experience, elaboration of the emotional dimension connected to this experience, elaboration of the life experiences linked to the relation with their relative).
Actions: “work schedule”
Problematic situation: Thoughts, emotions, and life experiences caused by the situation to the caregiver; response or consequence caused by the situation in the relationship between the caregiver and the patient.
Psychotherapeutic group: The emotions of the caregiver. Every caregiver expressed the real symptoms according to the discussed theme and according to the daily situations that are more stressful and harder to handle. Analysis of the strategies and of the behavioural, communicative, and emotional ways used by the caregiver in order to cope with these situations and confutation of the eventual wrong interpretations towards patients. Distinction of the effective strategies and of ineffective and unadaptable strategies. Elaboration of new relation ways and of more effective solutions for coping the situation.
Duration
Every group lasted 2 months for psychoeducational group. The psychotherapeutic groups had a meeting once a week lasting 90 minutes for 6 months.
Statistical analysis
The numerical data were expressed as median and range (minimum and maximum) and the categorical variables as absolute frequencies and percentage. Wilcoxon test was applied to assess the existence of significant differences, for each burden and for HDRS, between observation pre and post treatment. Some boxplots were realized in order to visualize the distribution of different kinds of burden and of HAM-D, pre- and post-treatment. The non-parametric rs Spearman correlation test was applied in order to assess the existence of significant interdependence between HAM-D, BURDEN, assistance time, and disease grade. Linear regression models were estimated in order to assess the influence of disease grade on each burden (time, evolutionary, physical, social, emotional and, likewise, total). Statistical analyses were performed using SPSS 22.0 for Window package. P-value smaller than 0, 05 was considered to be statistically significant. In all tables significant p-values were reported in bold.
Results
The results are shown in tables 1, 2, 3 and are divided into two phases, before and after participation, in psychoeducational and psychotherapeutic groups. As it can be seen in Table 1, the median age of the caregivers is 58 years, even if the range shows a strong variability of the data (which is however included between a minimum of 31 and a maximum of 79 years). The median schooling is 13 years, and this value indicates the achievement of the diploma for the majority of the examined caregivers. The median time of assistance provided is 9 hours and is included in a rather high variability range (1-22). Finally, the median score detected in the HAM-D test is quite high (22) and this result is destined to significantly decrease after psychotherapeutic treatment.
With respect to the categorical variables, referred to caregivers (Table 2) it is possible to note that the highest percentage (76%) is female; only 12% of the examined sample lost their job to devote themselves to the care of their family member; the most frequent family relationships are husband/wife in 48% of cases and son/daughter in 44%. The degree of illness for one’s relative is severe in 48% of cases or moderate in 32%. Finally, 68% of the examined caregivers live with the assisted family member. Focusing our attention on the effect of the psychotherapeutic treatment (Table 3 and Figure 1) it can be noted that for all the examined burdens (time, developmental, physical, social, emotional, and total) there is a significant reduction between the pre-treatment and post-treatment condition, as shown by the statistically significant p-values obtained by applying the Wilcoxon test. Also significant is the reduction in the score of the HAM-D test detected pre-treatment and post-treatment, passing from 22 to 13 (highly significant p-value). The most relevant data was the perceived level of restriction by the care giver: 80% of caregivers lived the assistance relation as a failure. The prevailing burden dimension was time burden and evolutionary burden; they also had a negative impact on mood. The time burden was directly and significantly related to the cognitive disturbance of the patient (b = 3.324; p = 0.041), such as verified by regression analysis.
By means of correlation analysis we obtained a significant positive interdependence between assistance time and degree of pathology (rs = 0.547; p = 0.005); the total perception of the care time burden was significantly and positively correlated with HAM-D (rs = 0.536; p = 0.006). The results also showed the existence of a significant and positive correlation between time dedicated to assistance and evolutionary burden (rs=0.458; p = 0.021) and, also, between degree of pathology and emotive burden (rs = 0.403; p = 0.0046). In the groups, the unpredictability and the wondering of the patient emerged, which made the relationship hard. The 90% of the delirious convictions in the 80% the aggressive or opposing behaviour and emotional instability cases, were seen as intentional and as cause of significant symmetries. From the burden we could relate to a statistically significant reduction in care burden (p > 0.001) between the first and second administration of the caregiver. Through experience in groups, psychoeducational programs have encouraged reflection, expression and containment of emotions, favoured by the dynamics of mirroring and solidarity that have been established between family members. In particular there was a major influence related to the emotional and social burden.
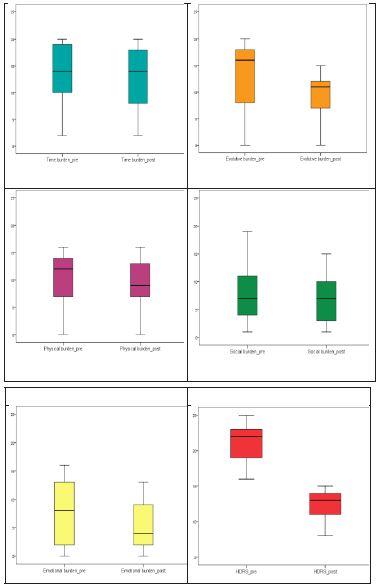
Table 1: Median and range of numerical variables referred to caregiver.
| Numerical Variables | Median | Range (min.–max.) |
|---|---|---|
| Age | 58 | 31-79 |
| Schooling (years) | 13 | 5-17 |
| Assistance time | 9 | 1-22 |
| HAM-D PRE | 22 | 7-25 |
| HAM-D POST | 13 | 6-21 |
Table 2: Absolute frequencies and percentages of categorial variables referred to caregiver.
| Categorical Variables | Frequencies | % | |
|---|---|---|---|
Sex |
Male Female |
6 19 |
24% 76% |
Lost work Relationship Degree of the disease Cohabitant |
Yes No Son/Daughter Husband/wife Son-in-law/ Daughter-in-law Low Moderate Severe Yes No |
3 22 11 12 4 |
12% 8% 44% 48% 8% |
| 5 8 12 |
20% 32% 48% |
||
| 17 8 |
68% 32% |
Table 3: Comparison pre and post treatment of the care burden and HAM-D (median, range and P- value).
| Objective | Pre | Post | P-value * |
|---|---|---|---|
| Time | 12 (2-20) | 14 (2-20) | 0.016 |
| Evolutive | 16 (0-20) | 11 (0-15) | < 0.001 |
| Physical | 12 (0-16) | 9 (0-16) | 0.003 |
| Social | 8 (1-19) | 7 (1-15) | 0.035 |
| Emotional | 8 (0-16) | 4 (0-13) | 0.001 |
| Total | 53.25 (8.25 – 88.25) | 4.25 (8.25-71.25) | < 0.001 |
| HAM-D | 22 (7-25) | 13 (6-21) | < 0.001 |
*P-values were obtained by means of Wilcoxon test.
Table 4: Results of linear regression model to evaluate the influence of disease degree on care burden.
| Dependent variables | Coeff. | S.E. | P-value |
|---|---|---|---|
| Time burden | 1.9 | 1.4 | 0.198 |
| Evolutive burder | 3.3 | 1.5 | 0.041 |
| Physical burden | 1.9 | 1.2 | 0.120 |
| Social burden | -0.9 | 1.4 | 0.539 |
| Emotional burden | 2.7 | 1.4 | 0.072 |
| Total burden | 9.0 | 5.2 | 0.099 |
Discussion and conclusion
In this study, thanks to the group’s work, the caregiver was helped to understand that the behaviours of the patient with dementia, defined as pathological, reflect the inevitable modifications caused by the illness in the relation between the subject and the surrounding environment. The brain damage and the consecutive involvement of the cognitive functions changes the patient affected by dementia, compared to who he/she was. This change determines a modification in the contents and in the interaction of the subject with his/her environment (people and things). For this reason, it is essential that the family member modifies his/her own relationship with his/her relative affected by dementia. Because “AD steals the mind”, the person that does not remember of a life spent with his/her relatives, feels robbed by his/her own life and also by his/her emotional life history. Therefore, it is fundamental that the family understands that there is a direct relation between the nature of the illness and the behaviour assumed by the patient. From the results of this study, it is clear that teaching to the caregivers how to cope with their relatives’ behavioural changes and personality in an effective way the daily life, reduces the level of stressand improves the life’s quality of both patients and caregivers. Flexibility, empathy, and creativity are the basic elements in order to cope with the assistance of patients with AD in a serene climate. The temptation of the current cultural world is that the dignity of the subject with dementia is dissolved, but the man, as a “person”, has his original dignity in every stage of existence. The patient with dementia is a “person” and in any relationship with him it’s worthy to recognize this dignity [29].
The approach to the patient with dementia must be based on a principle of sharing both goals and care plans. The needs analysis must be carried out within the “social care triangle”, a person with dementia- informal caregivers - formal caregivers, and it allows to cope with numerous ethical dilemmas that emerge during the course of the illness in compliance with the principles of autonomy, self-determination, charity, and social justice.
The capacity of each assistant to have an interpretative approach to the disease, with its set of cognitive and non-cognitive symptoms, is the guarantee of an adequate interpretation and management of behavioural disorders, for a better quality of life for all family members or for patients or caregivers.
Psychotherapists must be aware of their intrusion in a system which balance is threatened by the disease-driven change. Indeed, there is a painful anticipation of the loss both in the patient and in the caregiver, with a wide range of intense emotions and complex interactions. On the one hand, if without memory there is no self, on the other hand, whoever is not recognized by their beloved, after a life together, runs the risk of feeling deprived of their relationship and of their emotional background.
References
- Winblad B, Amouyel P, Andrieu S, et al. Defeating Alzheimer’s disease and other dementias: A priority for European science and society. Lancet Neurol. 2016; 15: 455-532.
- Hung YN, Kadziola Z, Brnabic AJ, et al. The epidemiology and burden of Alzheimer’s disease in Taiwan utilizing data from the National health insurance research database. Clinicoecon Outcomes Res. 2016; 8: 387-95.
- Alzheimer’s association. 2022.
- Gao Y, Liu X. Secular trends in the incidence of and mortality due to Alzheimer’s disease and other forms of dementia in China From 1990 to 2019: An age-period- cohort study and joinpoint analysis. Front. Aging Neurosci. 2021; 13: 709156.
- World Health Organisation. Dementia. 2019.
- Guerreiro R, Bras J. The age factor in Alzheimer’s disease. Genome Med. 2015; 7: 106.
- Aalten P, Jolles J, de Vugt ME, Verhey FR. The influence of neuropsychological functioning on neuropsychiatric problems in dementia. J. Neuropsychiatry Clin. Neurosci. 2007; 19: 50-56.
- Alzheimer’s Disease International. Overcoming the Stigma of Dementia. Available online: https://www.alz.co.uk/sites/default/files/pdfs/world-report-2012-summary-sheet.pdf
- Kales HC, Gitlin LN, Lyketsos CG. Assessment and management of behavioral and psychological symptoms of dementia. BMJ. 2015; 350: h369.
- Kaufer DI, et al. Assessing the impact of neuropsychiatric symptoms in Alzheimer’s disease: The Neuropsychiatric Inventory Caregiver Distress Scale. J. Am. Geriatr. Soc. 1998; 46: 210-215.
- Zahodne LB, Ornstein K, Cosentino S, Devanand DP, Stern Y. Longitudinal relationships between Alzheimer disease progression and psychosis, depressed mood, and agitation/aggression. Am. J. Geriatr. Psychiatry. 2015; 23: 130-140.
- Lanctôt KL, et al. Neuropsychiatric signs and symptoms of Alzheimer’s disease: New treatment paradigms. Alzheimers Dement. 2017; 3: 440-449.
- Lyketsos CG, et al. Neuropsychiatric symptoms in Alzheimer’s disease. Alzheimers Dement. 2011; 7: 532-539.
- Alves GS, Carvalho AF, de Amorim de Carvalho L, Sudo FK, Siqueira-Neto JI, et al. Neuroimaging Findings Related to Behavioral Disturbances in Alzheimer’s Disease: A Systematic Review. Curr Alzheimer Res. 2017; 14: 61-75.
- Brodaty H, Donkin M. Family caregivers of people with dementia. Dialogues Clin Neurosci. 2009; 11: 217-28.
- Murray ME, Graff-Radford NR, Ross OA, Petersen RC, Duara R, et al. europathologically defined subtypes of Alzheimer’s disease with distinct clinical characteristics: A retrospective study. Lancet Neurol. 2011; 10: 785-796.
- Petersen C, Nolan AL, de Paula França Resende E, et al. Alzheimer’s disease clinical variants show distinct regional patterns of neurofibrillary tangle accumulation. Acta Neuropathol (Berl). 2019; 138: 597-61.
- Okuda S, Tetsuka J, Takahashi K, Toda Y, Kubo T, et al. Association between sleep disturbance in Alzheimer’s disease patients and burden on and health status of their caregivers. J Neurol. 2019; 266: 1490-1500.
- Germain S, Adam S, Olivier C, et al. Does cognitive impairment influence burden in caregivers of patients with Alzheimer’s disease? J Alzheimers Dis JAD. 2009; 17: 105-114.
- Kolanowski A, Boltz M, Galik E, Gitlin LN, Kales HC, et al. Determinants of behavioral and psychological symptoms of dementia: A scoping review of the evidence. Nurs Outlook. 2017; 65: 515-529.
- Moyle W, Kellett U, Ballantyne A, Gracia N. Dementia and loneliness: An Australian perspective. Journal of Clinical Nursing. 2011; 20: 1445-1453.
- C Miranda-Castillo, B Woods, M Orrell. The needs of people with dementia living at home from user, caregiver and professional perspectives: A cross-sectional survey BMC Health Serv. Res. 2013; 13: 43.
- J Cohen-Mansfield, MS Marx, LS Freedman, H Murad, NG Regier, et al. The comprehensive process model of engagement Am. J. Geriatr. Psychiatry. 2011; 19: 859-870.
- McKhann G, Drachman D, Folstein M, Katzman R, Price D, et al. Clinical diagnosis of Alzheimer’s disease: Report of the NINCDS-ADRDA Work Group under the auspices of Department of Health and Human Services Task Force on Alzheimer’s Disease. Neurology. 1984; 34: 939-44.
- Novak M. e Guest C. Gerontologist. 1989; 29: 798-803.
- Adattata da Hamilton M. “Development of a rating scale for primary depressive illness.” British Journal of Social and Clinical Psychology. 1967; 6: 278-296.
- Morris JC. Clinical Dementia Rating: A reliable and valid diagnostic and staging measure for dementia of the Alzheimer type. International Psychogeriatrics. 1997; 9: 173176.
- Magni E, Binetti G, Bianchetti A, Rozzini R, Trabucchi M. Mini-Mental State Examination: A normative study in Italian elderly population. Eur. J. Neurol. 1996; 3: 198-202.
- Tomasello L. Toscano G. Raffaele M. Sacredness, dignity in Alzheimer’s disease Bioe-thos n.10 Bioethics Institute Privitera (Pa). 2021; 24-32.