
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 4
Secondary dysmenorrhea: Unicornuate uterus with rudimentary and non-communicating horn
*Corresponding Author : Patrícia Gomes Ferreira
Department of Obstetrics and Gynecology, Centro Hospitalar de Entre Douro e Vouga, Santa Maria da Feira, Portugal.
Email: patriciagomesferreira.10@gmail.com
Received : Aug 11, 2023
Accepted : Sep 04, 2023
Published : Sep 11, 2023
Archived : www.jcimcr.org
Copyright : © Ferreira PG (2023).
Abstract
Unicornuate uterus is a type of female genital malformation caused by abnormal development of Mullerian ducts during embryogenesis. Its prevalence is estimated to be close to 0.1%, 0.5%, and 2% in unselected women, infertile women, and those with a history of miscarriage, respectively [1]. Unicornuate uterus presents 4 subtypes based on the American Fertility Society Classification: up to 90% of cases have a rudimentary uterine horn, but only 25% are cavitated and noncommunicating [2].
We present a case of a young female patient with severe dysmenorrhea caused by hematometra in the rudimentary horn, which is not communicating with the uterine cavity. Our case falls into U4a class of ESHRE/ESGE classification and unicornuate with distal uterine remnant with functional endometrium class of ASRM Mullerian Anomalies Classification 2021 [3,4]. The diagnostic workup for these patients typically includes sonography and, whenever necessary, Magnetic Resonance Imaging (MRI) to better define which rudimentary horn variant is present and to evaluate the presence of associated renal anomalies [5].
Citation: Ferreira PG. Secondary dysmenorrhea: Unicornuate uterus with rudimentary and non-communicating horn. J Clin Images Med Case Rep. 2023; 4(9): 2586.
Description
A 32-year-old woman, nulligravida and not sexually active, was referred to the gynecology appointment with a chief complaint of a cyclic and severe pelvic pain, particularly at the time of her regular menses. The pain progressively increased over the last year, relieving slightly with non-steroidal anti-inflammatory drugs. She experienced menarche at the age of 15 years and had never had trouble during menstruation. She had never taken contraceptive or hormonal medication. She had no prior significant medical and family history.
The patient was hemodynamically stable. Gynecological examination revealed normal external genitalia. Speculum examination showed a single cervix with menstrual loss and no vaginal anomaly. Bimanual examination showed a uterus deviated to the right, with a tender mass on the left side with rebound but no rigidity or guarding. Transvaginal ultrasound examination showed a pelvic mass with 32 x 23 x 19 mm in the left adnexal area with isoechoic walls to the myometrium, containing hyperechoic material with ipsilateral hematosalpinx. These findings suggested a rudimentary and non-communicating horn (Figures 1 and 2). Subsequent pelvic MRI showed an anomalous uterine cavity with a single right-sided cornua communicating with the cervix, pushed to the right by a distended left-sided rudimentary horn with normal myometrial signal intensity (Figure 3). No concomitant renal anomaly was observed.
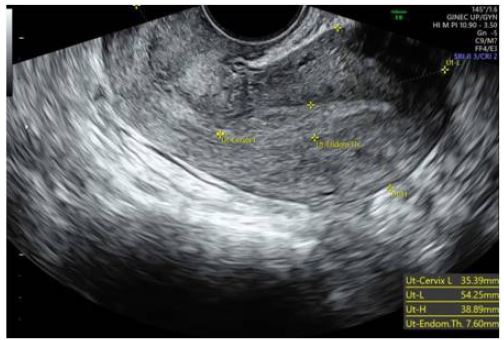

B. Rudimentary non-communicating horn with functioning cavity,
C. Hematosalpinx

B. Right unicornuate uterus,
C. Rudimentary non-communicating horn with functioning cavity.
References
- Ludwin A, Lindheim SR. Unicornuate uterus and the noncommunicating functional horn: Continued debate on the diagnosis, classification, and treatment. Fertil Steril. 2020; 113: 772-773.
- Sánchez-Ferrer ML, Prieto-Sanchez MT, Sánchez Del Campo F. Variations in clinical presentation of unicornuate uterus with non-communicating rudimentary horn (class IIB of the American Fertility Society classification). Taiwan J Obstet Gynecol. 2018; 57: 110-114.
- Grimbizis GF, Gordts S, Di Spiezio Sardo A, Brucker S, De Angelis C, et al. The ESHRE-ESGE consensus on the classification of female genital tract congenital anomalies. Gynecol Surg. 2013; 10: 199-212.
- Pfeifer SM, Attaran M, Goldstein J, Lindheim SR, Petrozza JC, et al. ASRM müllerian anomalies classification 2021. Fertil Steril. 2021; 116: 1238-1252.
- Khati NJ, Frazier AA, Brindle KA. The unicornuate uterus and its variants: Clinical presentation, imaging findings, and associated complications. J Ultrasound Med. 2012; 31: 319-31.