
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Acute monophasic disseminated encephalomyelitis due to enterococcus faecalis. Discussion of a case not described in the literature
Arroyo Antonio1,2*; Giglio Andrés1,2; Ferre Andrés1,2; Pedreros Cesar1,2; Kemeny Rodrigo1,2; Ramos Andrés1,2; Reccius Andrés1,2; Hasbún Pablo1,2; Dreyse Jorge1,2
1Finis Terrae University, Pedro de Valdivia 1509, Santiago, Chile.
2Critical Patient Center, Las Condes Clinic, Estoril 450, Las Condes, Santiago, Chile.
*Corresponding Author : Arroyo Antonio
Finis Terrae University, Pedro de Valdivia 1509, Santiago, Chile.
Email: antonio-gaa@hotmail.com &
antoniogaa@icloud.com
Received : Aug 14, 2023
Accepted : Sep 05, 2023
Published : Sep 12, 2023
Archived : www.jcimcr.org
Copyright : © Antonio A (2023).
Abstract
A 42-year-old male with chronic renal disease on peritoneal dialysis presented with a headache and altered consciousness. The patient developed fever, and the cerebrospinal fluid culture was positive for Enterococcus faecalis, leading to treatment with ampicillin and linezolid. Due to poor clinical outcomes, brain imaging revealed probable cerebritis, which was biopsied and found to be consistent with Acute Disseminated Encephalomyelitis (ADEM). Steroidal therapy was initiated with a favorable response.
This case report presents a literature review on monophasic ADEM secondary to enterococcal meningoencephalitis. This discussion focuses on the absence of previous descriptions of the coexistence of these two infrequent entities which are interrelated in this particular case.
Keywords: Meningoencephalitis; Enterococcus faecalis; Acute disseminated encephalomyelitis; ADEM.
Citation: Antonio A, Andrés G, Andrés F, Cesar P, Rodrigo K, et al. Acute monophasic disseminated encephalomyelitis due to enterococcus faecalis. Discussion of a case not described in the literature. J Clin Images Med Case Rep. 2023; 4(9): 2587.
Introduction
Acute Disseminated Encephalomyelitis (ADEM) is a monophasic demyelinating disease of the Central Nervous System (CNS) primarily associated with viral infections, although post-vaccination bacterial and parasitic etiologies have also been described [1]. It commonly presents in children under 10 years of age and in young adults, with an estimated prevalence of 0.3 to 0.8 per 100,000 individuals [2]. The condition manifests as multifocal neurological symptoms and encephalopathy, typically occurring within the first three months after the initial infection, resulting from focal brain demyelination [1,3].
The pathophysiology is presumed to be autoimmune, where myelin autoantigens, such as basic myelin protein, proteolipid protein, and oligodendrocyte myelin protein, share antigenic determinants with those of an infecting pathogen [4,5]. Microscopic examination revealed demyelination and perivascular inflammation, particularly perivenous inflammation. The inflammatory process shows the proliferation of microglial cells and mononuclear inflammatory infiltrates around veins and venules. Signs of vasculitis with infiltrates in the vessel walls, with or without necrosis, may also be observed [15]. The lesion areas showed myelin fragmentation and, in some cases, complete loss of myelin with relative preservation of axons [12,15].
Over the last 30 years, Enterococcus has become the third most common cause of nosocomial infections, with the emergence of resistance mechanisms that limit therapeutic options [6,7]. Enterococcal CNS infections represent between 0.3% and 4% of bacterial causes, predominantly in children, and are described in two clinical forms: post-neurosurgical and secondary to intra-abdominal infections with subsequent spontaneous bacteremia and subsequent CNS invasion [8,9].
Cases of Enterococcus CNS infection in adults showed a mean age of 57 years for spontaneous events, with a predominance of Enterococcus faecalis over feces in a 3:1 ratio. Most patients presented with fever (85%), meningeal signs (44%), altered consciousness (44%), headache (36%), and seizures (20%), with neurological sequelae of up to 23%, and a mortality rate of 26% [9].
Given the low incidence of these two pathologies and the absence of previous reports of ADEM secondary to Enterococcus CNS infection, we report this clinical case.
Clinical case
A 42-year-old male with a history of kidney transplantation with graft loss, peritoneal dialysis, and hypertension presented to the emergency department with a one-week history of holocranial headache and fluctuating consciousness. This condition was associated with dysfunction of the peritoneal catheter and inability to perform dialysis. The patient presented with a hypertensive crisis, tachycardia, afebrile, well perfused, and without respiratory distress. Neurological examination showed altered consciousness, characterized by alternating periods of moderate drowsiness and psychomotor agitation, without any motor or sensory disturbances, meningeal signs, or ocular, cranial nerve, or osteotendinous reflex alterations. Initial brain Magnetic Resonance Imaging (MRI) did not reveal any acute abnormalities, and laboratory tests showed increased nitrogen and inflammatory markers within the normal range (Table 1).
The initial diagnosis was uremic encephalopathy, and urgent hemodialysis was initiated. However, despite the improvement in systemic inflammatory markers and Cerebrospinal Fluid (CSF), the patient’s fluctuating neurological deficits persisted. After 48 h, the patient developed a fever. A lumbar puncture was performed, showing pleocytosis, low glucose, high protein levels, and gram-positive cocci in chains on Gram staining (Table 1). Based on these results, the antibiotic coverage was broadened to ceftriaxone plus vancomycin. CSF culture revealed Enterococcus faecalis, which is susceptible to multiple antibiotics, leading to the adjustment of the antibiotic regimen to ampicillin plus linezolid.
During the patient’s hospital course, he experienced a generalized tonic-clonic seizure and was transferred to the intensive care unit, which required invasive mechanical ventilation. Antiseizure therapy with levetiracetam was then initiated. Despite the normalization of electroencephalographic records, the patient continued to display a fluctuating pattern of agitation and moderate drowsiness after extubation. Follow-up neuroimaging (Figure 1) revealed a parieto-occipital right probable cerebritis focus, which increased in size on day 21. New CSF studies have shown a progressive decrease in pleocytosis and low glucose levels, with severe hyperproteinorrachia and negative culture results. Systemic autoimmune study results were negative. Considering the possibility of cerebral abscess or other complications, a cerebral biopsy was performed. Biopsy revealed increased cellularity due to numerous inflammatory cells involving the parenchyma and surrounding blood vessels, abundant macrophages clustered with small particles, loss of myelin on Luxol Fast Blue staining, and reactive gliosis in the adjacent parenchyma (Figure 2).
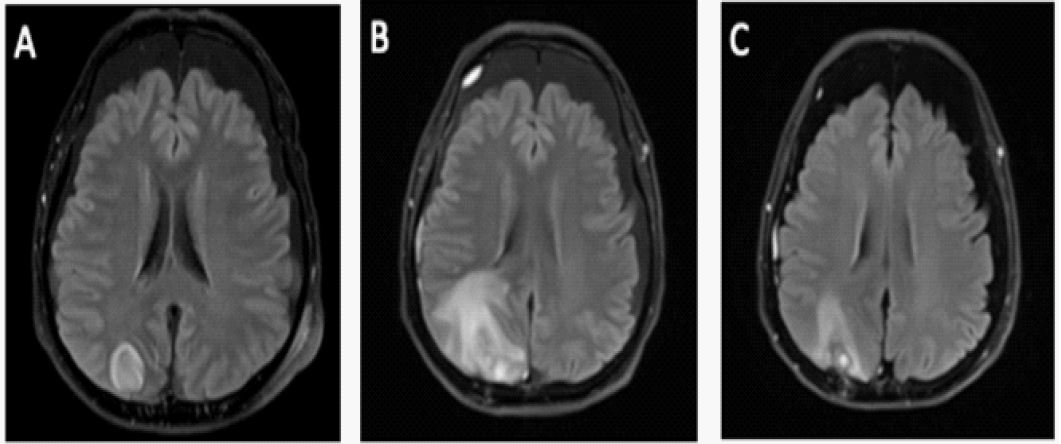
Figure 1B - Day 21 (MRI): Recent postsurgical (biopsy) changes in the right parietooccipital region, increased signal at the periphery of the lesion bed with a perilesional edema appearance larger than that observed in the study.
Figure 1C - Day 28 (MRI): Significant reduction of the lesion following high-dose methylprednisolone treatment.
Table 1: Evolutionary study of CSF.
| Study | Day 6 | Day 17 | Day 21 |
|---|---|---|---|
Lumbar Punction |
Leukocytes 150/mm3 Neutrophils 4% Glucose 10 mg/dl Proteins 624 mg/dl Lactate 5,6 mg/dl |
Leukocytes 62/mm3 Neutrophils 0% Glucose 43 mg/dl Proteins 730 mg/dl Lactate 4,6 mg/dl |
Leukocytes 23/mm3 Neutrophils 15% Glucose 42 mg/dl Proteins 602 mg/dl Lactate 5,3 mg/dl |
| CSF Crop | Enterococcus Faecalis no resistance profile | NEGATIVE | NEGATIVE |
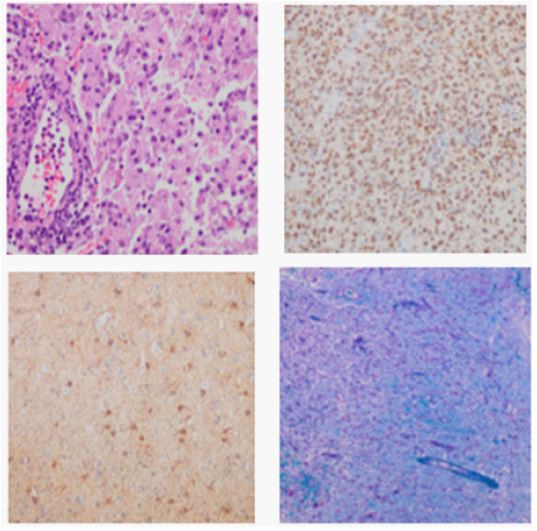
Microscopic Report: Sections demonstrate altered brain parenchyma architecture with increased cellularity due to numerous inflammatory cells involving the parenchyma and surrounding blood vessels. Abundant grouped macrophages were evident and contained small particles. Loss of myelin was observed using Luxol Fast Blue histochemical staining. Reactive gliosis was observed in the adjacent parenchyma.
Immunohistochemical Studies: CD68 is strongly positive in macrophages. Glial fibrillary acidic protein (GFAP) staining revealed numerous reactive astrocytes. CD3 is positive in numerous intraparenchymal and predominantly perivascular lymphocytes. CD20 revealed isolated positivity. Neurofilament reveals slight axonal edema. IDH-1 is negative.
Based on these findings and the clinical course, the patient was diagnosed with ADEM secondary to Enterococcus faecalis meningoencephalitis, and antibiotic treatment was continued for 37 days until negative biopsy cultures were obtained. Steroidal therapy was initiated with methylprednisolone 250 mg/day for three days, with a transition to prednisone, resulting in a favorable clinical response from the fifth day of corticosteroid therapy, and the patient gradually returned to his baseline condition.
Discussion
This case report describes the presentation of two infrequent interrelated diseases: Spontaneous meningoencephalitis caused by Enterococcus faecalis in adults with subsequent development of ADEM, definitively diagnosed through cerebral biopsy.
Nonspecific infectious symptoms associated with altered consciousness are the classic presentation described in reports of spontaneous meningoencephalitis caused by Enterococcus spp. in adults. Therefore, we suggest maintaining active suspicion and appropriate management of patients with risk factors for Enterococcus infection [9].
When fluctuating neurological focal deficits persist despite improvements in systemic and CSF inflammatory markers, the differential diagnosis should be extended to include alternative pathologies such as ADEM, where the appearance of white matter lesions accounts for nearly 85% of MRI findings, although approximately 80% of cases present with multifocal lesions. These MRI findings may initially be mistaken for focal infectious complications such as cerebritis and subsequent cerebral abscesses, which are more common [10]. Therefore, clinical and imaging evolution and potentially anatomopathological studies are essential for accurate diagnosis. The temporal aspect of ADEM development was consistent with our initial approach, in which a new MRI scan was performed on the 17th day of symptom persistence. However, the atypical presentation, both in the number of lesions and atypical bacterial infection, delayed the definitive diagnosis.
Identifying ADEM is crucial for the prognosis of these patients, as without timely treatment, neurological sequelae and mortality rates can reach up to 45% and between 8% and 25%, respectively [11]. In this patient, favorable clinical improvement occurred five days after initiating corticosteroids, leading to a return to his baseline consciousness level and subsequent intensive rehabilitation.
Notably, reported cases of ADEM are predominantly related to viral infections, while bacterial causes represent only 3% of all cases. In the literature review conducted by the authors, no cases associated with spontaneous Enterococcus infection were identified, making this the first reported case of the coexistence of both diseases.
References
- Scolding N. Acute disseminated encephalomyelitis and other inflammatory demyelinating variants. Handb Clin Neurol. 2014; 122: 601-11.
- Pohl D, Alper G, Van Haren K, Kornberg AJ, Lucchinetti CF, et al. Acute disseminated encephalomyelitis: Updates on an inflammatory CNS syndrome. Neurology. 2016; 87: S38-45.
- McAlpine D. Acute disseminated encephalomyelitis: Its sequels and its relationship to disseminated sclerosis. Lancet. 1931; 217: 846-52.
- Noorbakhsh F, Johnson RT, Emery D, Power C. Acute disseminated encephalomyelitis: clinical and pathogenesis features. Neurol Clin. 2008; 26: 759-80.
- Tenembaum S, et al. Acute disseminated encephalomyelitis. Neurology. 2007; 68: 23-36.
- Sood S, Malhotra M, Das BK, Kapil A. Enterococcal infections & antimicrobial resistance. Indian J Med Res. 2008; 128: 111-21.
- Guzman Prieto AM, van Schaik W, Rogers MR, Coque TM, Baquero F. Global Emergence and Dissemination of Enterococci as Nosocomial Pathogens: Attack of the Clones? Front Microbiol. 2016; 7: 788.
- Zhang X, Jiang C, Zhou C. Diagnosis of Enterococcus faecalis meningitis associated with long-term cerebrospinal fluid rhinorrhoea using metagenomics next-generation sequencing: A case report. BMC Infect Dis. 2021; 21: 1105.
- Pintado Vicente, Cabellos Carmen, Moreno Santiago, Meseguer María Antonia. Enterococcal Meningitis: A Clinical Study of 39 Cases and Review of the Literature. Medicine. 2003; 82: 346-364.
- Kajihara T, Nakamura S, Iwanaga N, Oshima K, Takazono T. Clinical characteristics and risk factors of enterococcal infections inNagasaki, Japan: a retrospective study. BMC infectious diseases. 2015; 15: 426.
- Li K, Li M, Wen L, Wang Q, Ding X. Clinical Presentation and Outcomes of Acute Disseminated Encephalomyelitis in Adults Worldwide: Systematic Review and Meta-Analysis. Front Immunol. 2022; 13: 870867.
- Vásquez P, Reccius A, Díaz M, Sáez L, Orellana P, et al. Encefalomielitis aguda diseminada de presentación atípica: utilidad de la biopsia estereotáctica para su diagnóstico. Caso clínico. Rev Med Chile. 2006; 134: 883-6.
- Ravin O, Hedley-White ET. A 55-year old man with cognitive and sensorimotor findings and intracranial lesions. N Engl J Med. 2002; 347: 1433-40.
- Peña AJ, Montiel NC, Herná ndez F, Medrano E, Valbuena O. Rev Neurol. 2002; 34: 163-8.
- Micheli F, Nogué s MA, Asconapé JJ, Ferná ndez PMM, Biller J. Tratado de neurologí a clí nica. 1ra. ed. Buenos Aires: Paname- ricana. 2002; 679-96.