
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Significant response to the combination of pyrotinib and capecitabine in a breast cancer patient with symptomatic and active brain metastases
Huihui Sun; Huimin Lv; Limin Niu; Min Yan*
Henan Breast Cancer Centre, The Affiliated Cancer Hospital of Zhengzhou University & Henan Cancer Hospital, Zhengzhou, China.
*Corresponding Author : Min Yan
Henan Breast Cancer Centre, The Affiliated Cancer Hospital of Zhengzhou University & Henan Cancer Hospital, Zhengzhou, China.
Email: ym200678@126.com
Received : Aug 15, 2023
Accepted : Sep 08, 2023
Published : Sep 15, 2023
Archived : www.jcimcr.org
Copyright : © Min Yan (2023).
Abstract
Background: Patients with Human Epidermal Growth Factor Receptor 2 (HER2)-positive breast cancer have a high risk of brain metastases. The combination of pyrotinib and capecitabine has shown the activity and safety among HER2-positive patients with brain metastases.
Case presentation: We report a case of one HER2-positive breast cancer patient with active brain metastases, who complained of headache and nausea. Pyrotinib plus capecitabine demonstrated significant efficacy for her intracranial lesions, while the symptoms were alleviated quickly and radiotherapy can be exempted temporarily.
Conclusion: The combination of pyrotinib and capecitabine can display efficacy quickly and continuously in HER2-positive breast cancer patients with symptomatic and active brain metastases.
Keywords: Breast cancer; Brain metastases; Pyrotinib; Case report.
Citation: Sun H, Lv H, Niu L, Yan M. Significant response to the combination of pyrotinib and capecitabine in a breast cancer patient with symptomatic and active brain metastases. J Clin Images Med Case Rep. 2023; 4(9): 2592.
Introduction
Breast cancer is the second most common primary tumor with brain metastases, and its incidence ranks only after non-small cell lung cancer [1]. Among the different molecular subtypes of breast cancer, the proportion of brain metastases in HER2 positive advanced breast cancer is the highest, about 30-55% [2,3]. Patients with brain metastases may experience intracranial hypertension, functional defects and irritating symptoms, such as dizziness and headache, nausea and vomiting, hearing and vision changes, and even hemiplegia and seizure, which are collectively referred to as symptomatic brain metastases [4].
At present, the clinical researches of brain metastases divide it into active brain metastases and stable brain metastases commonly. Active brain metastases include newly diagnosed brain metastases and progression brain metastases after previous local therapy, which are inclined to follow the imaging perspec.
LANDSCAPE was the first prospective study to assess medical treatment in HER2-positive breast cancer with active brain metastases. Forty-five patients with previously untreated brain metastases were included in this study to accept lapatinib and capecitabine, the results showed that the CNS Objective Response Rate (ORR) was 65.9% (57.1% RECIST1.0) and the Progression-Free Survival (PFS) was 5.5 months [6]. In HER2CLIMB, 118 patients with active brain metastases and 80 patients with stable brain metastases received the addition of tucatinib to trastuzumab and capecitabine, whose CNS-ORR was 47.3% (RECIST1.1), and the PFS was 9.9 months [7]. The above studies revealed the advantages of Tyrosine Kinase Inhibitor (TKI) drugs for active brain metastases. Seventy-eight women with active brain metastases was enrolled and treated with pyrotinib plus capecitabine in PERMEATE study [5]. The intracranial ORR was 74.6% (RECIST1.1) in 59 patients with radiotherapy-naive brain metastases and 42.1% in 19 patients with progressive CNS disease after radiotherapy. Moreover, the median PFS in radiotherapy-naive brain metastases was 11.3 months, and the treatment related adverse events were manageable.
Symptomatic brain metastases may cause some obvious negative experience to patients, thus limiting the strategy formulation and influencing the treatment outcome. When there was no effective medical therapy in the past, patients with symptomatic brain metastases would preferentially receive radiotherapy [8]. However, radiotherapy has noticeable adverse impact on the cognition, memory and quality of life of patients [9]. The combination of pyrotinib and capecitabine has showed a strong effect on HER2-positive active brain metastases, and patients could temporarily exempt from radiotherapy. Therefore, we provide a case report of symptomatic and active brain metastases, which show the significant response to the combination of pyrotinib and capecitabine and the process of symptom remission and tumor shrinkage, as a reference for clinical practice.
Case presentation
A 53-year-old postmenopausal woman with no significant familiar or medical history was initially diagnosed with a right breast cancer in 2020 (cT3N3M0). The pathology report revealed an ER-negative, PR-negative and HER2-positive invasive carcinoma of the breast. She received 7 cycles of anti-HER2-based neoadjuvant chemotherapy, and the efficacy reached partial response. Pruritus occurred after the first and second cycles of chemotherapy, so the chemotherapeutic drugs were replaced. She underwent modified radical mastectomy and the postoperative pathology reached the pathological Complete Remission (pCR) in March 2021, followed by adjuvant radiotherapy and targeted therapy for one year to October 2021. The specific time and drugs of systemic treatment before and after surgery were shown in Table 1.
On April 2, 2022, the patient sought MRI examination showed intracranial space occupation because she had suffered from headache and nausea for one week. On April 5, 2022, she came to our hospital in a wheelchair and Eastern Cooperative Oncology Group (ECOG) score was 3. After a thorough inspection, she was diagnosed with recurrence of breast cancer with active brain metastasis. Her symptoms were headache grade 3 and nausea grade 2 according to Criteria for Adverse Events (CTCAE) version 5.0. On the day of admission, we began to give symptomatic treatment using cimetidine, dexamethasone and mannitol. On April 6, the patient started pyrotinib 400 mg orally once daily without breaks, and capecitabine 1500 mg orally twice daily for 14 days, followed by 7 days off during each 21-day cycle. Surprisingly, the symptoms of headache and nausea were significantly relieved. By the time she was discharged from the hospital on April 15, she had only a slight headache and ECOG score decreased to 1. The hospitalization duration, drugs usage and changes in symptoms are recorded in Table 2. Taking the days of oral administration of pyrotinib and capecitabine as the time axis, the medication and symptom changes of patients are shown in Figure 1.
First imaging examinations (May 9, 2022) showed the maximum diameter of the two largest lesions shrunk remarkably (Figure 2A, 2B: from 34 to 17 mm; Figures 2E, 2F: from 19 to 8 mm) while the peritumoral brain edema had reduced significantly. Imaging findings suggested that the patient’s efficacy was evaluated as PR compared with the baseline brain MRI. The second (July 13, 2022) and third (September 13, 2022) reexamination proved the lesions were still shrinking and almost disappeared (Figures 2C 2D: 10 mm; Figures 2G 2H: 5 mm), the latest check (June 1, 2023) showed the lesions were stable, which indicated that the treatment has been effective for nearly 14 months. The patient had no obvious hematological toxicity, only grade 1 diarrhea and hand-foot syndrome, so no dose adjustment was required.
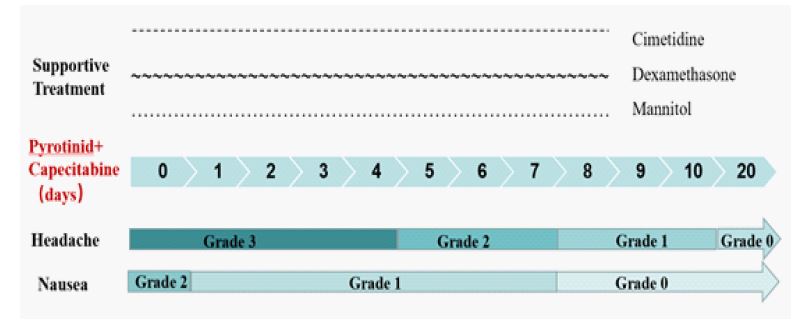

Table 1: Systemic treatment before and after surgery.
| Category | Date | Cycle | Treatment | Adverse events |
|---|---|---|---|---|
Neoadjuvant |
October 16, 2020 |
1 |
Docetaxel 126 mg Carboplatin 750 mg Trastuzumab 510 mg Pertuzumab 840 mg d1 q3w |
Pruritus |
November 6, 2020 |
1 |
Nab-paclitaxel 200 mg Carboplatin 750 mg Trastuzumab 378 mg Pertuzumab 420 mg d1 q3w |
Pruritus |
|
November 24, 2020- February 23, 2021 |
1-5 |
Vinorelbine 40 mg d1 d8 Carboplatin 750 mg Trastuzumab 378 mg Pertuzumab 420 mg d1 q3w |
Leukopenia |
|
Adjuvant |
March 23, 2021-October 29, 2021 |
1-11 |
Trastuzumab 378 mg Pertuzumab 420 mg d1 q3w |
None |
Table 2: The course of endoscopic treatments.
| Date | Symptom | Treatment | ||||
|---|---|---|---|---|---|---|
| Hospitalization | Headache | nausea | Symptomatic treatment | Anti-tumor therapy | ||
| April 5, 2022 | Grade 3 | Grade 2 | Cimetidine 200 mg qd ivgtt | Mannitol 50 g q12h | Dexame-thasone 5 mg qd iv | |
| April 6, 2022 | Grade 1 | pyrotinib 400mg qd +capecitabine 1500 mg bid d1-14 q3w | ||||
| April 7, 2022 | Mannitol 50 g q8h ivgtt | |||||
| April 10, 2022 | Grade 2 | |||||
| April 13, 2022 | Grade 1 | Grade 0 | ||||
| April 25, 2022 | Grade 0 | - | - | - | - | |
Discussion
Primary and metastatic brain tumors may be accompanied by peritumoral edema. Due to the limited intracranial space, peritumoral edema associated with tumors would further increase the encephalic pressure and aggravate clinical symptoms [10]. Steroids, specifically dexamethasone, have become the standard therapy for the management of tumor-associated edema [11,12]. As a hyperosmotic antihypertensive drug, mannitol can dehydrate and reduce encephalic pressure, and improve a series of neurologic symptoms resulting from intracranial hypertension [13]. For patients with severe symptoms, the dose and frequency of mannitol can be increased. Although other supportive treatments also can be used to target different symptoms specifically, the effective anti-tumor drugs are of uppermost priority. On the other hand, changes in patient’s symptoms can imply the effect of drugs earlier. If the symptoms are not relieved or even worsened, radiotherapy may have to be invoked. While the symptoms taking a turn for the better indicates that the anti-tumor drugs start working.
The adjuvant therapy for this case was standard and adequate, who treated with trastuzumab and pertuzumab for one year. Unfortunately, her tumor progressed significantly and brain metastases with symptoms occurred only half a year after the end of adjuvant treatment, which belonged to trastuzumab resistance. Pyrotinib is an oral irreversible pan-HER receptor TKI, PHENIX and PHOEBE studies have suggested the efficacy of pyrotinib combined with capecitabine in extracranial lesions, making it the standard second-line therapy in trastuzumab-treated HER2 positive advanced breast cancer in China [14,15]. And PERMEATE highlighted its effect in intracranial lesions [5]. Therefore, we recommended pyrotinib and capecitabine for this case. After one week of treatment, the symptoms were almost completely relieved, and the ECOG score was significantly reduced. One month later, the tumor had shrunk dramatically, and the diarrhea and hand-foot syndrome were tolerable. Up to now, the tumor has almost disappeared, and the adverse events were not aggravated. The patient came to the hospital for reexamination once every two months, and the rest of the time could return to the family and society, which is the goal and significance of our treatment.
For HER2-positive breast cancer with active brain metastases, in addition to TKI drugs, Antibody-Drug Conjugate (ADC) drugs have also achieved gratifying results. In the KAMILLA, 67 patients with brain metastasis treated with T-DM1 were active, with intracranial ORR of 49.3% [16]. Trastuzumab deruxtecan (T-DXd) showed surprising effects in advanced breast cancer patients with HER2 expression [17-19]. What’s more, TUXEDO-1 selected 15 HER2-positive breast cancer patients with active brain metastases, who were treated with T-DXd and their ORR reached 73.3% (RANO-BM) [20]. However, it should be noted that the ORR of 6 patients with de novo brain metastases was 100%, while that of 9 patients with progressed brain metastasis after radiotherapy was 66.7%, and PERMEATE also revealed the latter had a poorer response to drugs than the former. Besides, DEBBRAH designed five cohorts of patients with brain metastasis, among which the third cohort included 9 HER2-positive patients with progressed brain metastasis after local treatment. They received T-DXd treatment with an ORR of only 44.4% (RECIST1.1) [21]. These data implied that the response of intracranial lesions after radiotherapy to drug treatment was weakened and the efficiency was reduced. Therefore, different from the previous preference for intracranial radiotherapy, it is suggested to give priority to systemic treatment, and postpone the radiotherapy time as much as possible, which may better ensure the effectiveness of drug treatment and prolong the time of disease remission.
Blood Brain Barrier (BBB) is a tough problem in the treatment of brain metastases. Some studies on primary brain tumos suggested that tumor sites and mannitol drugs have limited role in opening the blood-brain barrier, while radiotherapy plays a certain role [11,22,23]. However, there is unanswered question about how and when does the radiotherapy work to open the BBB. And the damage of radiation to the hearing, vision, memory and cognitive ability of patients is irreversible to a large extent [9]. In addition, it should be noted that the ORR and PFS of patients who progressed after radiotherapy in PERMEATE and TUXEDO-1 were significantly lower than those with new brain metastases. Therefore, delaying the time of radiotherapy as much as possible may improve the efficacy of systemic treatment and prolong the survival of patients.
This case demonstrated that pyrotinib plus capecitabine has a rapid onset time, embodying in relieving symptoms and improving the status of patient quickly. And it has the ability to keep effective duration so that patients can delay suffering radiotherapy. This case provided more confidence and information to the treatment of symptomatic and active brain metastases.
References
- Lah TT, Novak M, Breznik B. Brain malignancies: Glioblastoma and brain metastases. Semin Cancer Biol. 2020; 60: 262-273.
- Niu L, Lv H, Zhang M, et al. Clinical diagnosis and treatment of breast cancer with brain metastases and establishment of a prognostic model: A 10-year, single-center, real-world study of 559 cases. Ann Transl Med. 2021; 9: 1331.
- Bailleux C, Eberst L, Bachelot T. Treatment strategies for breast cancer brain metastases. Br J Cancer.2021; 124: 142-155.
- Rostami R, Mittal S, Rostami P, et al. Brain metastasis in breast cancer: A comprehensive literature review. J Neurooncol. 2016; 127: 407-414.
- Yan M, Ouyang Q, Sun T, et al. Pyrotinib plus capecitabine for patients with human epidermal growth factor receptor 2-positive breast cancer and brain metastases (PERMEATE): A multicentre, single-arm, two-cohort, phase 2 trial. Lancet Oncol. 2022; 23: 353-361.
- Bachelot T, Romieu G, Campone M, et al. Lapatinib plus capecitabine in patients with previously untreated brain metastases from HER2-positive metastatic breast cancer (LANDSCAPE): A single-group phase 2 study. Lancet Oncol. 2013; 14: 64-71.
- Lin NU, Borges V, Anders C, et al. Intracranial Efficacy and Survival With Tucatinib Plus Trastuzumab and Capecitabine for Previously Treated HER2-Positive Breast Cancer With Brain Metastases in the HER2CLIMB Trial. J Clin Oncol. 2020; 38: 2610-2619.
- Ramakrishna N, Temin S, Chandarlapaty S, et al. Recommendations on disease management for patients with advanced human epidermal growth factor receptor 2-positive breast cancer and brain metastases: American Society of Clinical Oncology clinical practice guideline. J Clin Oncol. 2014; 32: 2100-2108.
- Chow E, Davis L, Holden L, et al. Prospective assessment of patient-rated symptoms following whole brain radiotherapy for brain metastases. J Pain Symptom Manage. 2005; 30: 18-23.
- Raizer JJ, Dixit KS. Managing Disease and Therapy-Related Complications in Patients with Central Nervous System Tumors. Curr Treat Options Oncol. 2015; 16: 38.
- Salvador E, Shityakov S, Förster C. Glucocorticoids and endothelial cell barrier function. Cell Tissue Res. 2014; 355: 597-605.
- Dixit KS, Kumthekar PU. Optimal Management of Corticosteroids in Patients with Intracranial Malignancies. Curr Treat Options Oncol. 2020; 21: 77.
- Bayir A, Kireşi DA, Kara H, et al. The effects of mannitol and melatonin on MRI findings in an animal model of traumatic brain edema. Acta Neurol Belg. 2008; 108: 149-154.
- Yan M, Bian L, Hu X, et al. Pyrotinib plus capecitabine for human epidermal growth factor receptor 2-positive metastatic breast cancer after trastuzumab and taxanes (PHENIX): A randomized, double-blind, placebo-controlled phase 3 study. Translational Breast Cancer Research. 2020; 1: 13-13.
- Xu B, Yan M, Ma F, et al. Pyrotinib plus capecitabine versus lapatinib plus capecitabine for the treatment of HER2-positive metastatic breast cancer (PHOEBE): A multicentre, open-label, randomised, controlled, phase 3 trial. Lancet Oncol. 2021; 22: 351-360.
- Montemurro F, Delaloge S, Barrios CH, et al. Trastuzumab emtansine (T-DM1) in patients with HER2-positive metastatic breast cancer and brain metastases: exploratory final analysis of cohort 1 from KAMILLA, a single-arm phase IIIb clinical trial. Ann Oncol. 2020; 31: 1350-1358.
- Cortés J, Kim SB, Chung WP, et al. Trastuzumab Deruxtecan versus Trastuzumab Emtansine for Breast Cancer. N Engl J Med. 2022; 386: 1143-1154.
- Shanu Modi, et al. ASCO abstract LBA3. 2022
- Modi S, Saura C, Yamashita T, et al. Trastuzumab Deruxtecan in Previously Treated HER2-Positive Breast Cancer. N Engl J Med. 2020; 382: 610-621.
- Bartsch R, Berghoff AS, Furtner J, et al. Trastuzumab deruxtecan in HER2-positive breast cancer with brain metastases: a single-arm, phase 2 trial. Nat Med. 2022.
- Batista et al. SABCS2021 PD4-06.
- Van Vulpen M, Kal HB, Taphoorn MJ, et al. Changes in blood-brain barrier permeability induced by radiotherapy: Implications for timing of chemotherapy? (Review). Oncol Rep. 2002; 9: 683-688.
- Wilhelm I, Molnár J, Fazakas C, et al. Role of the blood-brain barrier in the formation of brain metastases. Int J Mol Sci. 2013; 14: 1383-1411.