
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Research Article - Open Access, Volume 4
Assessing the epidemiological factors of epidermolysis bullosa in Shiraz, the referral center of Southern Iran
Ali Akbar Mohammadi1,2; Nasrin Saki3,4; Mohammad Mahdi Parvizi4; Amir Hossein Hassani5; Hossein Fatemian5; Mohammad Keshavarz5*
1Plastic Surgery, Wound Healing and Burn Research Center, Shiraz University of Medical Sciences, Shiraz, Iran.
2Division of Plastic and Reconstructive Surgery, Department of General Surgery, School of Medicine, Shiraz University of Medical Sciences, Shiraz, Iran.
3Department of Dermatology, School of Medicine, Shiraz University of Medical Sciences, Shiraz, Iran.
4Molecular Dermatology Research Center, Shiraz University of Medical Sciences, Shiraz, Iran.
5School of Medicine, Shiraz University of Medical Sciences, Shiraz, Iran.
*Corresponding Author : Mohammad Keshavarz
School of Medicine, Shiraz University of Medical Sciences, shiraz, Iran.
Tel: +989176354282;
Email: mkeshavarz93@gmail.com
Received : Aug 14, 2023
Accepted : Sep 08, 2023
Published : Sep 15, 2023
Archived : www.jcimcr.org
Copyright : © Keshavarz M (2023).
Abstract
Introduction: Epidermolysis Bullosa (EB) is an inheritable bullous disorder characterized by massive blistering of the skin in response to minor trauma. EB is classified into three types: EB Simplex, Junctional EB, and Dystrophic EB based on the level of tissue separation within the skin basement membrane.
Methods: This epidemiological study was carried out on all EB patients referred to dermatology clinics of Shiraz University of Medical Sciences, Iran, during 2017-2018.
Results: Of the 66 EB patients, 38 (57.57%) were male, and 28 (42.42%) were female. Six patients (9.09%) had EBS, 5 patients (7.57%) had JEB, and 55 (83.33%) had DEB. The incidence of this disease was 16 per one million. The mean age of the patients was 12.36 years. The average height and weight of the patients were 125.75 cm and 25.04 Kg, respectively in patients older than two years. The average head circumference of the children under two years old was 43.96 cm. According to EBDASI, five patients were in the mild group, 15 in the moderate group, and 46 in the severe group.
Conclusion: In conclusion, the high incidence of this disease in Fars province highlighted the importance of prenatal and preimplantation diagnosis by genetic methods.
Citation: Mohammadi AA, Saki N, Parvizi MM, Hassani AH, Keshavarz M, et al. Assessing the epidemiological factors of epidermolysis bullosa in Shiraz, the referral center of Southern Iran. J Clin Images Med Case Rep. 2023; 4(9): 2593.
Introduction
The term Epidermolysis Bullosa (EB) refers to a rare inherited disease characterized by different signs and symptoms. Based on the pattern by which blisters and erosions are formed in the different layers of skin, three types of EB are defined: Epidermolysis Bullosa Simplex (EBS; Epidermolytic); Junctional Epidermolysis Bullosa (JEB; Lucidolytic), and dystrophic Epidermolysis Bullosa (DEB, Dermolytic) [1]. Ever since EB was first defined, classification systems have been changed several times. In the newly revised classification system, which was published in 2008, Kindler syndrome, which is a mixed type of the disease, was introduced as the fourth type of inherited EB [2]. To date, over 30 distinctive subtypes have been diagnosed based on the phenotype, mode of inheritance, and genotype [3]. Each type and subtype have numerous extracutaneous genetically-based manifestations, which lead to quick and reliable diagnosis based on the disease presentation. The progress of disease varies from minimal blistering to life-threatening limitation of function [4]. Several complications have been described in EB patients, which provoke a lot of distress and decrease the quality of life. Complex and chronic involvements, including muscular dystrophy, gastrointestinal, pyloric atresia, and bone marrow disturbance, make the treatment more difficult to a level that it can lead to morbidity and even premature death [5]. In the absence of a specific treatment, the most important point about EB is principal care to manage blisters, prevent infection, and control complications. Before the conduction of any clinical trials to put the promising therapies under evaluation, determining the accurate incidence of the disease and its complications is of utmost importance. Consequently, this study aims to epidemiologically evaluate the complications and growth indices of EB patients in Fars, Iran.
Material and methods
This epidemiological study was carried out on all EB patients referred to dermatology clinics affiliated to Shiraz University of Medical Sciences, Iran, during 2017-2018. Comprehensive data collection was performed after several dermatologists confirmed the disease.
The Epidermolysis Bullosa Activity and Scoring Index (EBDASI) was used to evaluate the disease severity. Data regarding patients’ demographic information, past and current medical history, family history, growth indices, surgical history, and complications in the circulatory system, digestive system, integumentary system, lymphatic system, musculoskeletal system, nervous system, and urinary system were collected.
The data were analyzed using SPSS version 16.0 (SPSS, Chicago, IL, USA). The quantitative variables were reported as mean and standard deviation, and the qualitative variables were reported as frequency. P-values less than 0.05 were considered statistically significant.
Results
Demographic analysis
66 EB patients were evaluated: 38 patients (57.57%) were male, and 28 (42.42%) were female. Among the patients, 6 (9.09%) had EBS, 5 (7.57%) were afflicted with JEB, and 55 (83.33%) suffered from DEB. Most patients were from Fars province, with a small number from other provinces. The patients’ age ranged from one to 35 years, with a mean age of 12.36 ± 9.98 years and the median age of 10 years old. According to the last population census for Fars province, the incidence of EB was estimated to be 16 patients per million. Patients’ age distribution by EB type showed that DEB patients were the youngest, with a mean age of 11.45 years and a standard deviation of 9.64 years. However, the difference seen in the age of the patients in the three groups was not statistically significant (P>0.05). The simplex and the junctional group patients had a mean age of 12 and 9 years, respectively. The Sex distribution of the patients in the different groups was as follows: in the EBS group, 50% of the patients were male, and 50% were female (3 male and three female), 80% of the JEB patients were male, and the other 20% were female (4 male patients and one female patient), while around 56% of the DEB patients were male and 44% of them were female (31 male patients and 24 female patients).
Based on the Chi-Square test, no significant relation was seen between gender and EB types (P>0.05). The patients’ educational status were distributed as 24 patients (36%) were preschoolers, 32 patients (48.47%) were under diploma, five patients (7.57%) had high school diploma, three patients (4.54%) had bachelor’s degree, one patient (1.51%) had a Master’s degree, and one (1.51%) had Ph.D.
The growth indices for EB patients were recorded according to their age. The mean head circumference for 11 patients (less than two years of age) was calculated to be 43.96 ± 3.58 cm. The other 50 patients were evaluated based on their BMI. Severe thinness was seen in 31 (62% of the patients older than two years); 27 of them were afflicted with dystrophic EB, three with junctional EB, and one with simplex EB. Moderate thinness was seen in seven (14% of the patients older than two years) patients; one of them had simplex EB simplex, one had Junctional EB, and five had Dystrophic EB. Three patients had mild thinness (two with DEB, one with JEB). Only eight patients had normal weights (three simplex EB patients, five dystrophic EB patients). The average patients’ height and weight were 125.75 ± 32.04 cm and 25.04 ± 16.69 Kg, respectively.
Findings revealed that pruritus and dysphagia were the most frequent major complications in patients with EB. Other complications are detailed in the Table 1.
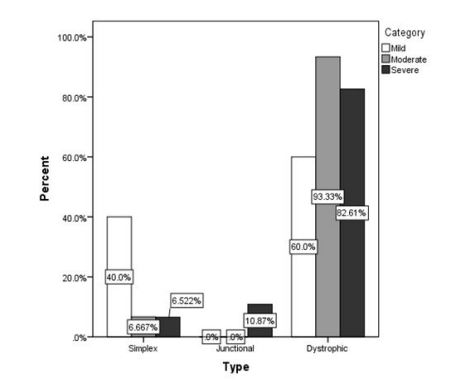
Table 1: Complications in different subgroups of EB.
| EBS | JEB | DEB | Total | |
|---|---|---|---|---|
| Circulatory system | ||||
| Heart Failure | 0 (0%) | 0 (0%) | 4 (100%) | 4 (6.06%) |
| Digestive system | ||||
| Dysphagia | 3 (6.25 %) | 3 (6.25%) | 42 (87.5%) | 48 (72%) |
| Pyloric atresia | 1 (5.88%) | 2 (11.76%) | 14 (82.35%) | 17 (25.75%) |
| GERD | 0 (0%) | 1 (7.14%) | 13 (92.85%) | 14 (21.21%) |
| Constipation | 1 (2.38%) | 4 (9.52%) | 37 (88.09%) | 42(63.63%) |
| Dental abnormalities | 3 (6.97%) | 4 (9.30%) | 36 (83.72%) | 43 (65.15%) |
| Endocrine system | ||||
| Delayed puberty | 0 (0%) | 0 (0%) | 4 (100%) | 4 (6.06%) |
| Integumentary system | ||||
| Pruritus | 3 (5.37%) | 5 (8.92%) | 48 (85.71%) | 56 (84.84%) |
| Infection | 3 (6.66%) | 5 (11.11%) | 37 (82.22%) | 45 (68.18%) |
| Chronic wound | 4 (7.54%) | 4 (7.54%) | 45 (84.90%) | 53 (80.30%) |
| Blisters | 4 (8.00%) | 4 (8.00%) | 42 (84%) | 50 (75.75%) |
| Erosions | 1 (4.16%) | 3 (12.5%) | 20 (83.33%) | 24 (36.36%) |
| Cancer | 0 (0%) | 0 (0%) | 2 (100%) | 2 (3.03%) |
| Lymphatic system | ||||
| Lymph Node Enlargement | 0 (0%) | 2 (10%) | 18 (90%) | 20 (30.30%) |
| Musculoskeletal system | ||||
| Bone mineralization | 1 (25%) | 0 (0%) | 3 (75%) | 4 (6.06%) |
| Flexion contractures | 1 (6.25%) | 0 (0%) | 15 (93.75%) | 16 (24.24%) |
| Distal trophic changes | 1 (4.16%) | 4 (16.66) | 19 (79.16%) | 24 (36.36%) |
| Acroosteolysis | 1 (5%) | 1(5%) | 18 (90%) | 20 (30.30%) |
| Muscular dystrophy | 1 (5.88%) | 1 (5.88%) | 15 (88.23%) | 17 (25.75%) |
| Nervous system | ||||
| Ears | 0 (0%) | 0 (0%) | 15 (100%) | 15 (22.72%) |
| Eyes | 2 (5.88%) | 2 (5.88%) | 30 (88.23%) | 34 (51.51%) |
| Respiratory system | ||||
| Nose | 1 (8.33%) | 1 (8.33%) | 10 (83.33%) | 12 (18.18%) |
| Upper airway | 0 (0%) | 0 (0%) | 3 (100%) | 3 (4.54%) |
| Stridor | 0 (0%) | 0 (0%) | 6 (100%) | 6 (9.09%) |
| Hoarseness | 1 (4.76%) | 1 (4.76%) | 19 (90.47%) | 21 (31.81%) |
| Urinary system | ||||
| Straining micturition | 0 (0%) | 1 (6.66%) | 14 (93.33%) | 15 (22.72%) |
| Meatal stenosis | 0 (0%) | 1 (25%) | 3 (75%) | 4 (6.06%) |
| Ulceratio | 0 (0%) | 3 (18.75%) | 13 (81.25%) | 16 (24.42%) |
| Urinary retention | 0 (0%) | 1 (33.33%) | 2 (66.66%) | 3 (4.54%) |
Severity analysis
According to the EBDASI guideline, the total EBDASI score ranges from zero to 506. The severity of the disease is classified as mild with scores ranging from zero to 42, moderate with scores ranging from 43 to 106, and severe with scores ranging from 107 to 506.
In the current analysis, patients were categorized as follows: five patients (7.57%) had mild disease, 15 (22.72%) had moderate EB, and 46 (69.69%) were suffering from severe EB. The mean age of the patients in different groups were 13.20 ± 13.73 years, 7.00 ± 6.09 years, and 14.02 ± 10.15 years, respectively.
The total mean for the EBDASI score of the patients was 14.42 ± 65.67 (ranging from 2 to 255). Since the EBDASI has separate scores for activity and damage, the mean score of the two subheadings was also calculated. It was found that the average score of the activity was 75.33 ± 41.99, and for the damage, it was 65.09 ± 30.56. Figure 1 presents the distribution of EB types based on the severity analysis.
Discussion
Epidermolysis Bullosa is an incurable and rare genetic disease defined by skin fragility and blisters that arise functional impairment, acute wounds, and infection. According to literature, EB can affect all racial and ethnic groups with no evidence for sex predominance [6].
Numerous incidence rates have been reported for EB since various factors such as the sampling method and the sample size affect the estimations. Although epidemiological techniques might be used as the gold standard for case finding, epidemiological estimates are influenced by sample size and sampling duration [7]. According to the last report of the National Epidermolysis Bullosa Registry, the incidence and prevalence of EB were estimated to be 19.57 and 11.07 cases per million, respectively, in a 16-year study. An increase was seen in the incidence rate of this disease; previously, the incidence rate was calculated to be 8.22 cases per one million live births [8]. Other reports about EB incidence were different; for example, the incidence of EB was 9.5 per million in Croatia, 8 per million in Italy, and approximately 10 per million in Europe [9]. The last report from National Registry estimated that 8 cases per one million population are afflicted with EB in Iran. It seems that despite the devastating consequences of this disease, it remains undiagnosed regularly.
In the present study, the predominant type of the disease was DEB (83%), the rate of which was impressively higher than similar studies in India (17%), Canada (35%), and Australia (35%) [10]. Also, controversial results were seen in the prevalence of Junctional EB among EB patients, estimated to be 7% in the current study, while lower prevalence was reported in the previous studies. Such significant differences prompt the need for a more accurate diagnosis.
EB imposes many extremely painful conditions on the patient, which require specific lifestyle modifications. The current study revealed that one of the most common complications of this disease is pruritus, which involves 84% of the patients. These results were similar to other studies. Gastrointestinal complications, especially dysphagia, were seen frequently in the present study (72%). This problem was usually reported as the sole complication of EB in previous studies. This problem causes a poor intake of nutrients and is associated with failure to thrive; therefore, severe thinness would be normal in EB patients. Moreover, bone mass is strongly associated with body size, and decreased bone mass was the main reason EB patients were significantly lighter and shorter than their peers without EB.
Since EB is an incurable disease and affects the quality of life, pain management is suggested to be the primary goal in approaching these patients. Codifying evidence-based pain care is highly recommended. Moreover, comprehensive management needs a multi-disciplinary team that consists of a dermatologist, a nutritionist, physical and occupational therapists, a surgeon, a dentist, a geneticist, and a psychologist to cover all aspects of EB disease. Unfortunately, due to a lack of genetic analysis equipment, we could not diagnose the subclasses of this disease, and it was a limitation for this study.
Conclusion
In conclusion, the high incidence of this disease in Fars province highlighted the importance of prenatal and preimplantation diagnosis by genetic methods. Since this disease has no definite treatment options, avoidance of giving birth to these patients is the main route of fighting this disease. Appropriate genetic counseling should be considered as an integral part of health care policies regarding this disease.
Limitations: Since the study was performed in Shiraz, Fars province of Iran, as a referral center of dermatological problems in South of Iran, the prevalence of the disease is most probably overestimated.
Declarations
Acknowledgements: We thank all the patients and their families who cooperated in this study. This article is retrieved from the MD dissertation of Dr. Mohammad Keshavarz. AAM and MK designed the study. NS, MMP, AHH, HF, and MK collected the data; AAM, MMP, AHH, and HF analyzed the data; MK, and AHH prepared the first draft of the manuscript, all of the authors revised the manuscript.
Funding information: No fund
Conflict of interest: All the author declare no conflict of interest.
Consent statement: All of the participants or their legal guardians consented to enter the study and to have their information published if remained anonymous and if the data were reported collectively.
References
- Watkins J. Diagnosis, treatment and management of epidermolysis bullosa. British Journal of Nursing. 2016; 25: 428-431.
- Fine JD, et al. Inherited epidermolysis bullosa: Updated recommendations on diagnosis and classification. Journal of the American Academy of Dermatology. 2014; 70: 1103-1126.
- Marzano AV, et al. Diagnosis and disease severity assessment of epidermolysis bullosa acquisita by ELISA for anti‐type VII collagen autoantibodies: An Italian multicentre study. British Journal of Dermatology. 2013; 168: 80-84.
- Vorobyev A, RJ Ludwig, E Schmidt. Clinical features and diagnosis of epidermolysis bullosa acquisita. Expert review of clinical immunology. 2017; 13: 157-169.
- Fine JD, JE Mellerio. Extracutaneous manifestations and complications of inherited epidermolysis bullosa: Part I. Epithelial associated tissues. Journal of the American Academy of Dermatology. 2009; 61: 367-384.
- Intong LR, DF Murrell. Inherited epidermolysis bullosa: New diagnostic criteria and classification. Clinics in dermatology. 2012; 30: 70-77.
- Boeira VL, et al. Inherited epidermolysis bullosa: Clinical and therapeutic aspects. An Bras Dermatol. 2013; 88: 185-98.
- Fine JD. Epidemiology of Inherited Epidermolysis Bullosa Based on Incidence and Prevalence Estimates From the National Epidermolysis Bullosa Registry. JAMA Dermatol. 2016; 152: 1231-1238.
- Pavicic Z, et al. Occurrence of hereditary bullous epidermolyses in Croatia. Pediatr Dermatol. 1990; 7: 108-10.
- Kho YC, et al. Epidemiology of epidermolysis bullosa in the antipodes: The Australasian Epidermolysis Bullosa Registry with a focus on Herlitz junctional epidermolysis bullosa. Arch Dermatol. 2010; 146: 635-40.