
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Short Report - Open Access, Volume 4
Eight-year chronic wound caused by Tarlov’s cyst
Ya-Ning Huang1; I-Wei Chang2; Sung-Tse Li1,3,4; Wei-Te Lei1*
1Department of Pediatrics, MacKay Memorial Hospital, Hsinchu, Taiwan.
2Department of Pathology, Taipei Medical University Hospital, Taipei, Taiwan.
3Department of Medicine, MacKay Medicine College, New Taipei, Taiwan.
4Department of Healthcare Management, Yuanpei University of Medical Technology, Hsinchu, Taiwan.
*Corresponding Author : Wei-Te Lei
Department of Pediatrics, MacKay Memorial Hospital, Hsinchu, Taiwan.
Tel: 886-03-6119595; 0975837110; 03-6119595;
Email: Weite.lei@gmail.com
Received : Aug 19, 2023
Accepted : Sep 12, 2023
Published : Sep 19, 2023
Archived : www.jcimcr.org
Copyright : © Wei-Te L (2023).
Citation: Ya-Ning H, I-Wei C, Sung-Tse L, Wei-Te L. Eight-year chronic wound caused by Tarlov’s cyst. J Clin Images Med Case Rep. 2023; 4(9): 2599.
Short report
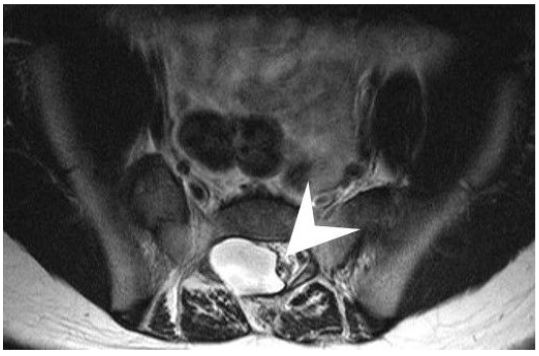
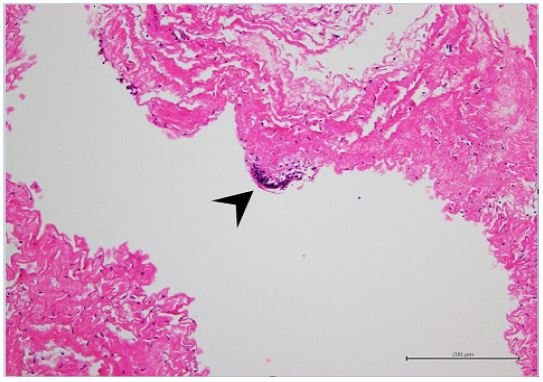
A 10-year-old girl presented with eight-year history of chronic osteomyelitis. She could walk without assistance until two years old and was found to fall over easily until now. She was seemed to be not sensitive to pain. Since one and a half years old, she started to suffer from recurrent toes cellulitis and was refractory to antibiotics treatment even with afebrile condition, slightly elevated white cell counts and erythrocyte sedimentation rate. Furthermore, she received five times of sequestrectomy at two, three, five, seven and nine years old, respectively. As a result, her big toes were amputated due to persistent chronic osteomyelitis (Figure 1). Nevertheless, the immune function tests were all normal. Neurological examination revealed that she has blunt sensation in L4 and L5 dermatome, especially at bilateral forefoot area and diminished L4 deep tendon reflex. She also presented slapping gait pattern owing to inadequate muscle power of tibialis anterior which was innervated by deep peroneal nerve coming from posterior tibia part of sciatic nerve (L4-S3). Magnetic Resonance Imaging (MRI) demonstrated a lobulated cyst at the right aspect of the S1-S3 canal about 1.8 cm x 0.5 cm in size and no nerve root was contained within the cyst (Figure 2A). Tethered conus syndrome (Figure 2B) along with neurogenic bladder is highly suspected. Urodynamic study confirmed the diagnosis of neurogenic bladder. Finally, she received Laminectomy of L5 and S1-S2 which led to the diagnosis of right S1-S3 epidural cyst. The tethering effect of S1-3 epidural cyst which contributed to slapping gait is compatible to innervation of posterior tibia part of sciatic nerve (L4-S3). The final diagnosis from the histopathological examination was right S1-3 Tarlov’s cyst (Figure 3). The clinical condition of diminished sensation and gait pattern had much improved after successful surgical treatment.
Tarlov’s cyst, also known as perineural cyst, is cerebrospinal-fluid-filled sacs. It usually forms on the extradural component of sacrococcygeal nerve roots at the junction of dorsal root ganglion and posterior nerve roots [1]. It often locates at the S1 to S5 nerve root area which caused corresponding radiculopathy, paresthesia and muscular weakness. Most of Tarlov’s cysts are asymptomatic until it become larger enough to cause stretching or compression effect to the nerve root, which is mostly known as tethered conus syndrome [2,3]. Therefore, perineural cyst is often underdiagnosed since it is difficult to identify without image assistance. Among the two types of Tarlov’s cyst, the one located next to the nerve tissue often causes less symptoms in early life, compared with the cyst located posterior to the root ganglion with nerve fibers inside. The difference course of disease progress is due to the extent of compression to the nerve root [4]. Besides, some studies found out that neuropathic anesthesia in the lower limbs are caused by spinal cord compression associated with spinal bony defect [5]. As in our case, the type of cyst which no nerve root was containing inside caused longer period to make the correct diagnosis. Considering the difficulty to make timely diagnosis, careful review of imaging study which revealed symptomatic cyst is crucial for timely diagnosis.
In children who present recalcitrant chronic wound accompanied with slapping gait pattern and foot hypoesthesia to pain, aggressive image examination such as spine MRI should be arranged for further evaluation especially when the children are immunocompetent. Early detection and diagnosis of symptomatic Tarlov’s cyst with tethered conus syndrome assist the child to preserve neurologic function and life quality.


Supplement 1: Thoracolumbar scoliosis. Butterfly vertebra of T8. Height decrease in T5 to T9 vertebral bodies.
Supplement 2: Hypoplasia of posterior elements in L3 to L5 vertebrae.
References
- Tarlov IM. Spinal perineurial and meningeal cysts. J Neural Neurosurg Psychiatry. 1970; 33: 833-43.
- Feigenbaum F, Henderson F. Tarlov cysts. In: Benzel E, editor. Spine surgery. 3rd ed. Philadelphia (PA): Elsevier. 2012; 1135-40.
- Ju CI, Shin H, Kim SW, Kim HS. Sacral perineural cyst accompanying disc herniation. J Korean Neurosurg Soc. 2009; 45: 185-7.
- Nabors MW, Pait TG, Byrd EB, Karim NO, Davis DO, et al. Updated Assessment and Current Classification of Spinal Meningeal cysts. J Neurosurg. 1988; 68: 366-7.
- Pedro EB, Juan AZ. Painless leg and moving toes syndrome due to spinal cord compression. J Eur Spine. 2008; 17: 294-295.