
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 4
A deeper look behind the cutaneous nodules
Danay Pérez Mijenes*; João Caiano Gil
Internal Medicine Department, Hospital Pedro Hispano, Unidade Local de Saúde de Matosinhos, Senhora da Hora, Portugal.
*Corresponding Author : Danay Pérez Mijenes
Internal Medicine Department, Hospital Pedro Hispano, Unidade Local de Saúde de Matosinhos, Senhora da Hora, Portugal.
Email: danaypm@yahoo.es
Received : Sep 02, 2023
Accepted : Sep 18, 2023
Published : Sep 25, 2023
Archived : www.jcimcr.org
Copyright : © Mijenes DP (2023).
Citation: Mijenes DP, Gil JC. A deeper look behind the cutaneous nodules. J Clin Images Med Case Rep. 2023; 4(9): 2611.
Description
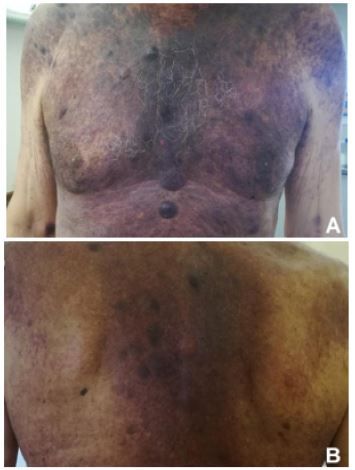
A 72-year-old male was referred to our outpatient clinic due to the appearance of cutaneous lesions 3 months earlier, asthenia, anorexia and a loss of 5% of body weight. The physical examination showed brownish macules primarily located in the torso region (Figures 1A,B), which progressed to painful and tense purple nodules with hematic content, distributed predominantly on the face and upper limbs. Laboratory studies revealed pancytopenia, with evidence of immature neoplastic haematological cells in peripheral blood immunophenotyping. A skin biopsy was performed, with histology examination suggestive of dendritic plasmacytoid cells leukaemia. Further staging studies demonstrated spinal involvement, leukemic dissemination, ocular involvement, and a diffuse ganglion. He completed an intensive chemotherapy regimen with cyclosphosphamide, doxorubicin, vincristine and prednisolone; but without signs of clinical relapse, culminating in the death of the patient 9 months after the diagnosis.
Blastic plasmacytoid dendritic cell neoplasm (BPDCN) is a rare, aggressive neoplasm arising from precursors of type 2 or plasmacytoid dendritic cells, usually associated with poor outcomes [1]. The median age at presentation is approximately 70 years and they are male [2]. Most patients with BPDCN present with skin lesions with or without bone marrow involvement and leukaemic dissemination, however the acute leukaemic form accounts for < 1% of cases [3]. The skin lesions may be brown to purple, similar to ecchymoses, plaques or tumours as shown in the image, and may be solitary or disseminated [1,5]. Skin biopsy with histology and routine immunophenotyping is the most important laboratory test to establish the diagnosis [4,5]. After chemotherapy, the average survival time is about 12-14 months, and only patients who undergo allogeneic stem cell transplantation achieve long-term remission [3,4]. The authors emphasise the importance of high clinical suspicion for diagnosis, especially in patients who present with skin lesions and cytopenias.
References
- Julia F, Petrella T, Beylot-Barry M, Bagot M, Lipsker D, Machet L et al. Blastic plasmacytoid dendritic cell neoplasm: clinical features in 90 patients. Br J Dermatol. 2013; 169(3): 579-86.
- Lim MS, Lemmert K, Enjeti A. Blastic plasmacytoid dendritic cell neoplasm (BPDCN): a rare entity. BMJ Case Rep. 2016. PMID: 26791132
- Pagano et al. Blastic plasmacytoid dendritic cell leukemia. Blastic plasmacytoid dendritic cell neoplasm with leukemic presentation: an Italian multicenter study. Haematologica. 2013; 98(2).
- Sweet K. Blastic plasmacytoid dendritic cell neoplasm: diagnosis, manifestations, and treatment. Curr Opin Hematol. 2020; 27(2): 103-107.
- Jain A, Sweet K. Blastic Plasmacytoid Dendritic Cell Neoplasm. J Natl Compr Canc Netw. 2023; 21(5): 515-521.