
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Multisystemic embolization as first manifestation of infective endocarditis: A case report
Danay Pérez Mijenes1*; Susana Viana1; João Caiano Gil1; Emmanuel Neves2
1Internal Medicine Department, Hospital Pedro Hispano, Unidade Local de Saúde de Matosinhos, Senhora da Hora, Portugal.
2Ophthalmology Department, Hospital Pedro Hispano, Unidade Local de Saúde de Matosinhos, Senhora da Hora, Portugal.
*Corresponding Author : Danay Pérez Mijenes
Internal Medicine Department, Hospital Pedro Hispano, Unidade Local de Saúde de Matosinhos, Senhora da Hora, Portugal.
Email: danaypm@yahoo.es
Received : Sep 02, 2023
Accepted : Sep 19, 2023
Published : Sep 26, 2023
Archived : www.jcimcr.org
Copyright : © Mijenes DP (2023).
Abstract
Infective endocarditis is a severe and rare disease that remains a diagnostic and treatment challenge nowadays. A high index of suspicion and low threshold for investigation are essential to the prompt institution of antibiotic therapy. Extracardiac manifestations, generally due to emboli, must not be forgotten and may be the first manifestation of the disease. Early surgery is a mainstay in cases of high risk of embolization. We present the case of a 63-year-old man with a history of mitral valve prolapse, that was admitted to the hospital for three days evolution of behavioral changes. The initial study revealed a recent cerebral ischemic infarction and bilateral areas of infarction of the kidneys. Echocardiogram showed vegetation of the mitral valve and Streptococcus anginosus was isolated in blood cultures; therefore, infective endocarditis was diagnosed. The patient evolves with multiple ocular embolic lesions and endogenous endophthalmitis and underwent early cardiac surgery.
Keywords: Endocarditis; Endophthalmitis; Streptococcus Anginosus; Embolization.
Citation: Mijenes DP, Viana S, Gil1 JC, Neves E. Multisystemic embolization as first manifestation of infective endocarditis: A case report. J Clin Images Med Case Rep. 2023; 4(9): 2613.
Background
Infective endocarditis (IE), initially described more than 350 years ago, is an infection of the endocardium of the heart which may include one or more heart valves [1]. The clinical manifestations of IE are protean and can involve every organ system. Embolic phenomena are common and can affect up to 50% of individuals with IE [1,4]. While cardiovascular complications are the most common in IE, clinicians should be aware of extracardiac manifestations which may result from septic embolism including endogenous endophthalmitis (EE) [4]. Multidisciplinary care is essential to the best management of IE.
Case description
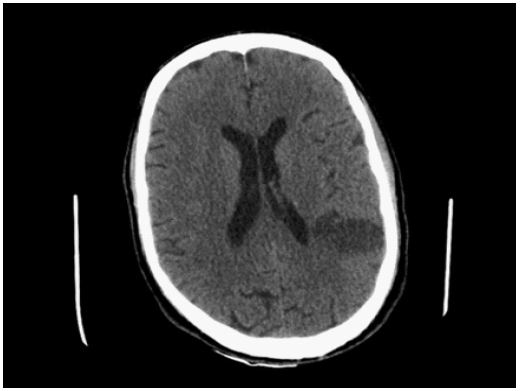
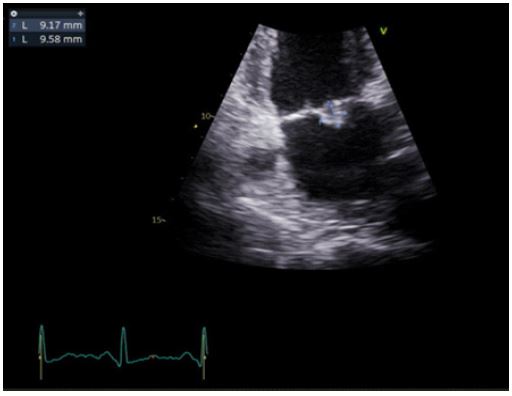
A 63-year-old man with a past medical history of mitral valve prolapse conditioning moderate mitral valve regurgitation, was admitted to the emergency department for three days of evolution of behavioral changes with psychomotor slowing, disorientation, and confusion. Anamnesis also revealed asthenia and weight loss of 15 Kg in three months. On admission, he was apyretic, hemodynamically stable, and disoriented, with no focal deficits on neurological examination or other objective alterations. Laboratory tests revealed anemia of 12.2 g/dL, thrombocytopenia of 123,000 platelets/uL, leukocytosis of 16,700 leukocytes/uL with neutrophilia of 15,200/uL and C-reactive protein of 149 mg/L. A brain computed tomography (CT) showed a left parietal cortico-subcortical infarction sequelae [Figure 1] and a thoracoabdominopelvic CT was performed to search for an infectious focus, which revealed bilateral renal infarcts, without a mass or obvious focus of infection. The study was continued with a lumbar puncture that demonstrated cerebrospinal fluid (CSF) with 40% glucose consumption, 95 mg/dL protein, and pleocytosis of 224 cells/uL - 55% of polymorphonuclear cells. It was started empiric antibiotic therapy for central nervous system infection with ceftriaxone and ampicillin. No agent was isolated on CSF. Because of findings of multiple ischemic lesions, transthoracic and transesophageal echocardiograms were performed that revealed a 13x5 mm vegetation on the mitral valve with friable appearance and findings suggestive of perforation of the anterior leaflet of the mitral valve, without significant valve functional impairment (Figure 2). Streptococcus group anginosus was isolated in blood cultures. The diagnosis of IE was made, and antimicrobial therapy was de-escalated for ceftriaxone in accordance with the agent isolated. He completed the study with Magnetic Resonance Imaging (MRI) of the brain which only revealed the previously described ischemic lesion with characteristics suggesting a recent infarction. MRI angiography had no signs of mycotic aneurysms.
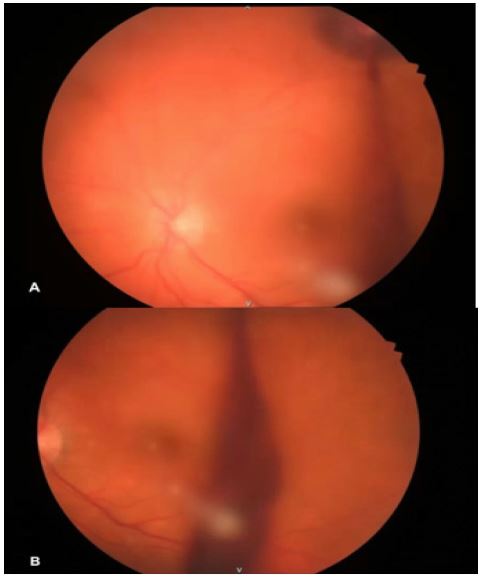
The next day, the patient developed visual symptoms of floaters and decreased visual acuity in his left eye. Examination of the ocular fundus revealed a dense vitreous haemorrhage and a round, subretinal haemorrhage found along the course of the superior temporal retinal artery. This lesion displayed a white centre (Roth’ spot), as well as active bleeding (Figure 3), explaining the vitreous haemorrhage. Considering the likely infectious etiology, the patient was initially submitted to intravitreal injections of vancomycin and ceftazidime, but due to a rapidly deteriorating course (i.e., increase in the number of Roth’ spots and signs of vitritis), he was submitted to pars plana vitrectomy for EE. This patient was diagnosed with IE of the native mitral valve. As complications of the disease, the patient presented perforation of the anterior leaflet of the mitral valve and multisystemic embolization: cerebral, renal, and ocular, with associated EE and meningitis by hematogenous dissemination. Due to the severity of the case with documented active multisystemic embolization, the patient was transferred to the hospital of reference, where he underwent valve replacement surgery of the mitral valve. He also underwent a vitrectomy of his left eye.
Discussion
IE is an infection of the endocardium, that typically involves the heart valves or an intracardiac device [1]. It is a rare and severe disease, but it maintains a poor prognosis despite improvements in diagnostic testing, antibiotic therapy, and surgical treatment [1-3]. Rapidly it can cause cardiac and extracardiac injury, and it can involve every organ system by migration of embolic material through arterial circulation [1]. Its clinical presentation is highly diverse from acute sepsis to an indolent febrile illness, heart failure, or stroke [3]. In this case, the patient had a nonspecific clinical presentation and the clinical suspicion of IE was raised by the signs suggestive of cerebral and renal ischemic events in the exams performed.
The main etiological agents for IE are Staphylococci and Streptococci [1,3]. However, IE caused by the Streptococcus anginosus group is infrequent and accounts for less than 10% of cases of IE caused by Streptococcus viridians [6].
Embolic events can affect up to 50% of patients with IE. The brain is one of the most frequent sites of embolization, with rates of IE complicated with a stroke in 20-40% of cases. The risk of embolization is highest during the first week and it can occur before admission, but the risk is substantially reduced with initiation of antibiotic therapy [1-3]. The classic ocular manifestation of infective endocarditis is Roth’s spot (hemorrhages with white centers), but recent studies have shown that they are only present in 2% of patients [4]. Our patient evolves with another ocular complication, EE, a rare ocular inflammatory manifestation of IE that affects the intraocular structures, as a result of migration of septic emboli and hematogenous dissemination of microorganisms [5]. It is associated with high mortality rates and poor visual prognosis [4]. Streptococcus is the most common agent group [5] and S. anginosus should be considered in the differential diagnosis of slowly progressive endogenous endophthalmitis [5]. Prompt administration of antibiotic therapy is the key in the acute management of EE, and empiric broad-spectrum antibiotic therapy with vancomycin and aminoglycoside or a third-generation cephalosporin is recommended [5]. The role of intravitreal antibiotics and vitrectomy is still not well defined, but they have a role in cases that progress despite medical therapy [5].
The indications and the optimal timing for surgical treatment in IE are not consensual, especially when cerebral complications occur [3]. However, if indicated, it should preferably be considered early in the course of the disease and not delayed [1,2]. This decision should be made by a multidisciplinary team for better outcomes. In this patient, early cardiac surgery was essential. He presented a vegetation of more than 10 mm involving the anterior mitral leaflet with a friable appearance as a risk factor for embolism and evidence of multiple embolic events with active embolization under antibiotic therapy.
Conclusion
Making a rapid and accurate diagnosis when IE is suspected is a key challenge in this disease. This case highlights the extracardiac complications of endocarditis, which are often the first manifestation of the disease because of their severity, and the fact that they were associated with EE. It is crucial to emphasize a multidisciplinary approach in IE, not only in the management of the disease but also in IE research.
References
- Hubers SA, DeSimone DC, Gersh BJ, Anavekar NS. Infective Endocarditis: A Contemporary Review. Mayo Clin Proc. 2020; 95(5): 982-997.
- Wang A, Fosbøl EL. Current recommendations and uncertainties for surgical treatment of infective endocarditis: a comparison of American and European cardiovascular guidelines, European Heart Journal. 2022 May; 43(17): 1617-1625.
- Cahill TJ, Baddour LM, Habib G, Hoen B, Salaun E, et al. Challenges in Infective Endocarditis. J Am Coll Cardiol. 2017; 69(3): 325-344.
- Villasmil RJ, Lattanzio N, Burns K, Alkayali T. More Than Meets the Eye: Infective Endocarditis Presenting as Endogenous Endophthalmitis. Cureus. 2021; 13(4): e14745.
- Francisco Ramón Breijo-Marquéz, editor. Endocarditis. Croatia: InTech. 2011.
- Escrihuela-Vidal F, López-Cortés LE, Escolà-Vergé L, González ADA, Cuervo G, et al. Clinical Features and Outcomes of Streptococcus anginosus Group Infective Endocarditis: A Multicenter Matched Cohort Study. Open Forum Infect Dis. 2021; 29; 8(6): ofab163.