
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Shrinking lung syndrome: A pulmonary complication of systemic lupus erythematosus
Danay Pérez Mijenes*; João Caiano Gil
Internal Medicine Department, Hospital Pedro Hispano, Unidade Local de Saúde de Matosinhos, Senhora da Hora, Portugal.
*Corresponding Author : Danay Pérez Mijenes
Internal Medicine Department, Hospital Pedro Hispano, Unidade Local de Saúde de Matosinhos, Senhora da Hora, Portugal.
Email: danaypm@yahoo.es
Received : Sep 04, 2023
Accepted : Sep 19, 2023
Published : Sep 26, 2023
Archived : www.jcimcr.org
Copyright : © Mijenes DP (2023).
Abstract
Shrinking lung syndrome (SLS) is a rare and underrecognized complication of systemic lupus erythematosus (SLE) that can occur at any point in the disease. Several etiologies have been proposed, but the exact pathophysiologic mechanism has not been established. We report the case of a 47-year-old female patient with SLE, who presents exertional dyspnea with pleuritic chest pain. A SLS was diagnosed and a prompt treatment was initiated in order to reduce long-term morbidity and mortality and maintain the quality of life.
Keywords: Shrinking lung syndrome; Diaphragm dysfunction; Systemic lupus erythematosus.
Citation: Mijenes DP, Gil JC. Shrinking lung syndrome: A pulmonary complication of systemic lupus erythematosus. J Clin Images Med Case Rep. 2023; 4(9): 2614.
Introduction
SLS is a rare manifestation of SLE characterized by decreased lung volumes and diaphragmatic weakness in a dyspneic patient [1]. A low threshold of clinical suspicion and the use of careful testing are required to allow timely diagnosis after exclusion of other clinical entities. Therapeutic regimens based on corticosteroids, immunosuppressants, and beta-agonists are used with apparent clinical improvement.
Case description
A 47-year-old Caucasian female sought the emergency department because of dyspnea and chest pain. She had a 6-year history of SLE. This diagnosis was based on clinical - arthritis of small and medium joints - and immunological - positive antinuclear antibodies (1:2560, speckled pattern), double-stranded DNA (dsDNA), Ro/SSA and La/SSB antibodies, low C3 and normal C4 serum levels - criteria.
The Systemic Lupus Erythematosus Disease Activity Index 2000 (SLEDAI-2K) was 0 after being on standard of care therapy (hydroxychloroquine, methotrexate up to 20 mg/week) and steroids (maximum dose of 10 mg of prednisolone).
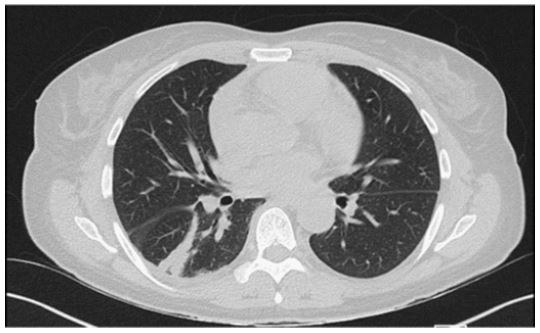
She reported 1-month evolution of exertional dyspnea and pleuritic chest pain that worsened with decubitus. There was no history of trauma or infection. A cardiovascular or pericardial diseases were excluded (no electrocardiographic alterations or myocardial necrosis markers elevation were documented; no segmental kinetic alterations of the ventricles or indirect signs of pulmonary hypertension were observed on echocardiography). There was no respiratory failure. The blood cell count and imumunologic analysis revealed normochromic normocytic anemia (hemoglobin 9.7 g/dL, without vitamins deficiency), increased dsDNA levels, complement consumption, increased sedimentation rate of 86 mm/h (N<30 mm/h) and mild increase in C-reactive protein (18 mg/L, N<5 mg/L). Chest radiograph showed smaller lung volume with raised right hemidiaphragm (Figure 1); computed tomography angiography revealed predominantly basal atelectasis, with no changes in lung parenchyma or images suggestive of thromboembolism (Figure 2). Negative result for SARS-CoV-2 testing were obtained by real time-polimerase chain reaction.
Pulmonary function tests (PFT) were performed which showed severe restrictive ventilatory failure (forced vital capacity (FVC) 26% of predicted, forced expiratory volume in one second (FEVE1) 33% of predicted, and diffusion capacity of the lungs for carbon monoxide (DLCO) 21% of predicted), with ultrasound studies confirming marked limitation of movement (consistent with paresis of the bilateral hemidiaphragm), with thickening of both hemidiaphragms less than 10%. Involvement of the first or second motor neuron was excluded (myositis panel, brain, and axial MRI showed no relevant changes).

A diagnosis of exclusion, Shrinking lung syndrome, was made. A high dose of oral prednisolone (0.5 mg/kg/day) and an inhaled beta-2 agonist were started with a gradually favorable clinical response. However given the severe restrictive effect and the need to consolidate the favorable results, the patient started immunosuppressive therapy with mycophenolate mofetil, which allowed descending corticosteroid therapy. The patient showed improvement in her symptoms and follow up PFT revealed better results (FVC of 41% of predicted, FEV1 48%, and DLCO 34%).
Discussion
Shrinking lung syndrome is a rare complication of systemic lupus erythematosus, first described by Hoffbrand and Beck in 1965 [2,3]. This uncommon entity affects between 0.5% and 1.53% of all lupus cases and is usually diagnosed 4 years after the onset of SLE [2,4].
Several etiologies have been proposed, but the exact pathophysiologic mechanism has not yet been demonstrated due to the rarity of reported cases and lack of research [2-4]. It is possible that myopathy or myositis of the diaphragm leads to muscular dysfunction; however, this hypothesis contrasts with some reports that suggest normal diaphragmatic function in most patients with SLS [1]. Another hypothesis postulates damage or paralysis of the phrenic nerve. Some other reports suggest a possible role of chronic pleural inflammation in altered pulmonary compliance [4,5].
The biggest challenge in diagnosing SLS is the nonspecificity of the symptoms and the relative innocence of the tests. Patients usually manifest shortness of breath, chest pain, normal lung parenchyma, restrictive ventilatory defect, and elevation of the diaphragm, despite the absence of other pulmonary pathologies such as interstitial, alveolar, or pulmonary disease [5]. These constellations of signs, symptoms and diagnostic teste led us to the diagnosis of SLS in our patient.
Glucocorticoid therapy and other immunosuppressants have been reported to improve both pulmonary function and symptoms [2,5]. The efficacy of theophylline or other beta-adrenergic agonists remains controversial, but the potential beneficial effect in this situation is likely due to their positive inotropic capacity on the diaphragm, as has been observed in animals [5]. In this report, the patient received an initial therapeutic regimen of glucocorticoids and inhaled beta-2 agonist, with subsequent favorable clinical evolution and improvement of PFT, and posterior consolidation of the regimen after introduction of immunosuppression with mycophenolate mofetil.
Conclusion
The authors point out the importance of increasing awareness for early recognition of this entity when the underlying cause of shortness of breath with raised hemidiaphragm is unclear. Early diagnosis and prompt treatment play an important role in preventing the disease progression and improving the morbidity and mortality.
References
- Roy F, Korathanakhun P, Karamchandani J, Dubé BP, Landon-Cardinal O, Routhier N et al. Myositis with prominent B-cell aggregates causing shrinking lung syndrome in systemic lupus erythematosus: a case report. BMC Rheumatol. 2022; 6: 11.
- Smyth H, Flood R, Kane D, Donnelly S, Mullan RH. Shrinking lung syndrome and systemic lupus erythematosus: a case series and literature review. QJM. 2018; 111: 839-843.
- Henderson LA, Loring SH, Gill RR, Liao KP, Ishizawar R, Kim S et al. Shrinking Lung Syndrome as a Manifestation of Pleuritis: A New Model Based on Pulmonary Physiological Studies. J Rheumatol. 2013; 40: 273-28.
- Depascale R, Del Frate G, Gasparotto M, Manfrè V, Gatto M, Iaccarino L et al. Diagnosis and management of lung involvement in Ther Adv Musculoskelet Dis. 2021; 13: 1759720X211040696.
- Haji Datoo A, Abdelghani L. Shrinking Lung Syndrome: A Case Report. Cureus. 2022; 14(7): e27311.