
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Giant Bowen’s disease on the anterior abdomen: Lull before the storm
*Corresponding Author : Rajesh Rajagopalan
Senior Consultant Dermatovenereologist, Department of Skin, STDs and Leprosy, KMCH Speciality Hospital, Erode, Tamilnadu, India.
Email: rajrajskin@yahoo.co.in
Received : Sep 05, 2023
Accepted : Sep 22, 2023
Published : Sep 29, 2023
Archived : www.jcimcr.org
Copyright : © Rajagopalan R (2023).
Abstract
Background: Bowen’s disease is a rare and unusual premalignant skin condition. It commonly present as large scaly erythematous patch or plaque, often giving rise to a large spectrum of differential diagnoses especially in hidden areas.
Case presentation: We report an elderly male patient with Bowen’s disease on the right hypochondrium and epigastric region which was successfully removed by wide excision.
Conclusion: We report this case to draw attention to the necessity of the self-skin examination in the geriatric population so as to prevent development of invasive squamous cell carcinoma from long standing skin diseases. Dermoscopy often confirm the diagnosis as non-invasive tool. We highly recommend mandatory excision in all cases and topical imiquimod 0.5% in cases who refuse or unfit for surgery.
Keywords: Bowen’s disease, Large size, Atypical site, Histopathology, Wide excision.
Citation: Rajagopalan R. Giant Bowen’s disease on the anterior abdomen: Lull before the storm. J Clin Images Med Case Rep. 2023; 4(9): 2620.
Introduction
Bowen’s disease (BD) is a rare, progressive, intraepithelial neoplastic condition first described by John Templeton Bowen in 1912 [1]. The risk of development of invasive carcinoma is 3%-5% in extra genital lesions and 10% in genital lesions [2]. It commonly occurs over sun‑exposed areas such as head, neck and lower limbs. Clinically, it presents as single well‑defined erythematous plaques mimicking psoriasis or eczema. Multiple site disease, hidden area involvement is seen in chronic arsenic intoxication [3,4]. Here, we report a case of elderly male patient of BD with occurrence over rare site.
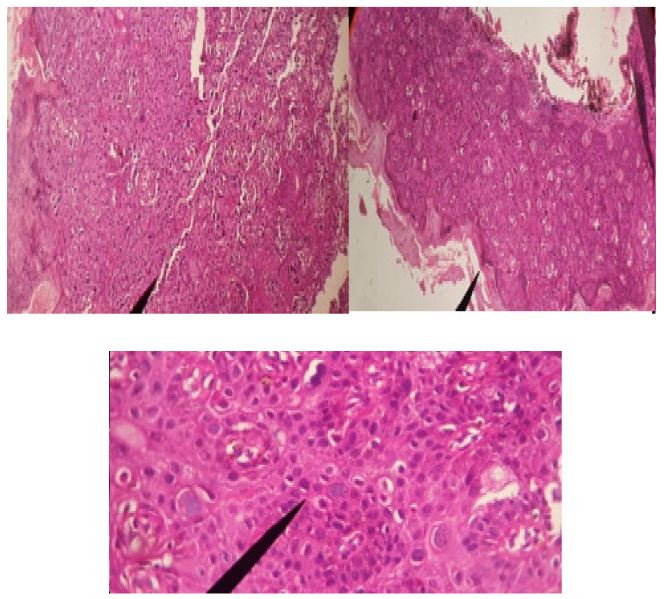
A 65-year-old farmer was referred to our OPD with a history of slowly enlarging scaly erythematous lesion on the front of abdomen, over the last four years. Minimally itchy and was managed elsewhere as eczema or psoriasis with no relief. No H/O of previous cutaneous carcinomas in the past or in family members. No H/O of using well water for drinking or cooking purposes. After meticulous clinical and dermoscopic examination of the entire body skin, no other lesions were noticed. Local dermatological examination revealed large scaly, slightly elevated dry dull red plaque of size 5x4.5 cm with well-demarcated borders from the surrounding healthy skin over right hypochondrium and epigastric region (Figure 1). Dermoscopic findings through the surface of the entire lesion showed glomerular/dotted vessels and yellow-white opaque scales on an erythematous background, suggestive for Bowen’s disease. Histopathological examination revealed parakeratosis in stratum corneum with atypicality in cells throughout the epidermis. Individual dyskeratotic cells and increased mitotic figures were seen in the stratum spinosum (Figure 2a,b,c). With confirmation of diagnosis, we did wide elliptical excision with 1 cm clearance. Margins (excisional biopsy report) were free of squamous atypia. Patient is under follow up for 1 year with no local recurrence or development of new lesions elsewhere in the body.

Discussion
Bowen’s Disease usually occurs over sun exposed sites. Giant disease although not uncommon is rarely reported [5]. “large Bowen’s disease” as a lesion with a dimension more than 2 cm and Lopez et al [6]. Used the term “extensive Bowen’s disease” for those lesions larger than 3 cm in diameter [7]. Our patient had dimensions (5x4.5 cm). Dermoscopic findings were strongly suggestive for Bowen’s disease and ruled out eczema or psoria sis in our case. Histopathology being gold standard confirmed our dilemma. To have fully blown disease, period varies between 2-40 years which confirms slow, lateral spread warranting late presentation in the OPD. The most common location of giant Bowen’s disease as per literature is the abdomen, followed by flanks. These are sun non exposed (cloth covered parts) of the body. Hidden area should make one suspect chronic arsenic exposure (food or water). Our patient did not have high levels of serum arsenic (less than 1 μg per dL). The concentration of total arsenic in urine was also within normal limits (≤50 mcg/L). Although most of the lesions are asymptomatic with cosmetic concern, they may be itchy and pose difficulty in diagnosis as clinical features overlap with dermatological conditions such as seborrheic keratosis, superficial basal cell carcinoma, actinic keratosis, eczema, tinea corporis, chronic plaque psoriasis, seborrheic dermatitis etc. Long standing uncared Bowen’s disease often advances to invasive SCC. Treatment modalities for Bowen’s disease are topical agents such as 5% 5 fluorouracil 5% imiquimod, cryotherapy, curettage, photodynamic therapy with 5-Aminolevulinic acid (ALA), radiotherapy, and ablative lasers.Last but not the least surgical excision is the curative therapy. The therapeutic choice can be influenced by the age, number, size and location of the lesion, preferable and comfortable solution by the patient and affordability of the therapeutic modalities [8].
Conclusion
We suppose that large size of the disease is due to neglecting the skin lesion by the patient or family members due to old age of the patient leading to late diagnosis and management. Therefore a self-skin examination in this elderly age group will be ideal due to increasing prevalence of cutaneous cancers. Dermoscopic examination as a non-invasive tool should be done in all long standing red atypical skin plaques to rule out mimickers, which also help to choose the best site for biopsy. Early recognition and timely surgical management (wide excision), long term follow up for local recurrence is the need of the hour.
Declarations
Declaration of patient consent: The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship: Nil
Conflicts of interest: There are no conflicts of interest
References
- Singh S, Khaitan BK, Sharma MC, Seenu V, Kumawat M, Chatterjee P. Bowen’s disease on finger: A diagnostic and therapeutic challenge. Indian J Dermatol Venereol Leprol 2013; 79: 227-30.
- Kao GF. Carcinoma arising in Bowen’s disease. Arch Dermatol. 1986; 122: 1124-1126. https://doi.org/10.1001/archderm.1986.01660220042010 PMid:3767398.
- Gahalaut P, Rastogi MK, Mishra N, Chauhan S. Multiple pigmented Bowen’s disease: A diagnostic and therapeutic dilemma. Case Rep Oncol Med 2012; 2012: 342030.
- Cöl M, Cöl C, Soran A, Sayli BS, Oztürk S. Arsenic-related Bowen’s disease, palmar keratosis, and skin cancer. Environ Health Perspect. 1999; 107(8): 687-9. doi: 10.1289/ehp.107-1566498. PMID: 10417369; PMCID: PMC1566498.
- Bakardzhiev I, Chokoeva AA, Tchernev G. Giant extragenital Bowen’s disease. WienMedWochenschr. 2015; 165(23-24): 504- 7.https://doi.org/10.1007/s10354-015-0396-z PMID:26542410.
- Morton CA, Whithurst C, McColl JH, et al. Photodynamic therapy for large or multiple patches of Bowen’s disease and basal cell carcinoma. Arch Dermatol. 2001; 137: 319-324. PMid:11255332.
- Lopez N, Meyer-Gonzales T, Herrera-Acosta E, et al. Photodynamic therapy in the treatment of extensive Bowen’s disease. J Dermatol Treat. 2012; 23: 428-430.https://doi.org/10.3109/09546634.2011.590789 PMid:21787214.
- Morton CA, Birnie AJ, Eedy DJ. British Association of Dermatologists’guidelines for the management of squamous cell carcinoma in situ (Bowen’s disease) 2014. British Journal of Dermatology. 2014; 170: 245-260.