
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
An unexpected cause of refractory thrombocytopenia in post renal transplant patient
Navneet Mishra1; Sabina Langer2*; Bhalla AK3; Nitin Gupta4; Jyoti Kotwal2
1Senior Resident, Department of Haematology, Sir Ganga Ram Hospital, Rajinder Nagar, New Delhi, India.
2Pathology, Senior Consultant, Department of Haematology, Sir Ganga Rama Hospital, Rajinder Nagar, New Delhi, India.
3Medicine, Senior consultant, Department of Nephrology, Sir Ganga Ram Hospital, Rajendra Nagar, New Delhi, India.
4Clinical Hematology and BMT, New Delhi, India.
*Corresponding Author : Sabina Langer
Pathology, Senior Consultant, Department of Haematology, Sir Ganga Rama Hospital, Rajinder Nagar, New Delhi, India.
Email: sabinapost@yahoo.com
Received : Sep 08, 2023
Accepted : Sep 25, 2023
Published : Oct 02, 2023
Archived : www.jcimcr.org
Copyright : © Langer S (2023).
Abstract
Post renal transplant patient often present with cytopenias including thrombocytopenia, this could be multifactorial including the immunosuppressive drugs, viral infections. Patient need immediate supportive treatment. The underlying etiology needs to be identified and treated. One of the less suspected cause is opportunistic infection like disseminated histoplasmosis. Progressive disseminated histoplasmosis is an uncommon opportunistic infection, largely affecting immunocompromised individuals, among organ transplant patients most commonly occur in post kidney transplant and patients on calcinurin inhibitor. The initial manifestation are fever, weight loss, hepatosplenomegaly, thrombocytopenia to an acute, rapidly fatal course causing resp. failure, shock, coagulopathy and multiorgan failure. Diagnosis can we made by histoplasma antigen assay or demonstration of histoplasma among tissue and bone marrow biopsy. Treatment include Intravenous amphotericin B with Long term itraconazole. We present an interesting case of disseminated histoplasmosis in post renal transplant patient presented with rashes, bleeding manifestation and severe thrombocytopenia, interestingly thrombocytopenia not responding to platelet transfusion, intravenous immunoglobulins and intravenous corticosteroids.
Citation: Mishra N, Langer S, Bhalla AK, Gupta N, Kotwal J. An unexpected cause of refractory thrombocytopenia in post renal transplant patient. J Clin Images Med Case Rep. 2023; 4(10): 2624.
Introduction
Renal transplantation faces a risk of developing various blood disorder including post-transplant anemia, post-transplant lymphoproliferative disorder, erythrocytosis, post-transplant cytopenias thrombotic microangiopathy, treatment related – Myelodysplastic syndrome. Among them thrombocytopenia is quite prevalent in 1st year after transplantation. Thrombocytopenia occurs as result of bone marrow suppression due to immunosuppressant agent, post-transplant infection, acute rejection episode, chemotherapy, nutritional deficiency of Vitamin B12 and folic acid. Among infection cytomegalovirus and Epstein Bar virus infection are quite common other are histoplasma capsulatum and Leishmania donovani that can manifest in immunocompromised state. Histoplasma Capsulatum is thermal dimorphic fungus, endemic in north and South America particularly the Mississippi and ohio river valleys. Infectious form is mycelia, shortly after infection mycelia transform into the yeast that found inside macrophage and other phagocyte. Soil enriched with bird/bat dropping promote the growth and sporulation of histoplasma [1]. Population at risk of histoplasmosis continues to grow as a result of increase number of patient receiving immunosuppressive therapies for autoimmune disorder, cancer, organ transplant clinical spectrum of Histoplasmosis is from asymptomatic infection to life threatening illness.
Progressive Disseminated Histoplasmosis (PDH) is mainly seen in immunocompromised host. Common clinical features are fever, weight loss, hepatosplenomegaly, thrombocytopenia to an acute, rapidly fatal course causing resp. failure, shock, coagulopathy and multiorgan failure.
This report present an unusual case of disseminated Histoplasmosis in renal allograft recipient patient that presented with petechial rash, epistaxis and gum bleeding bleeding manifestation.
Case report
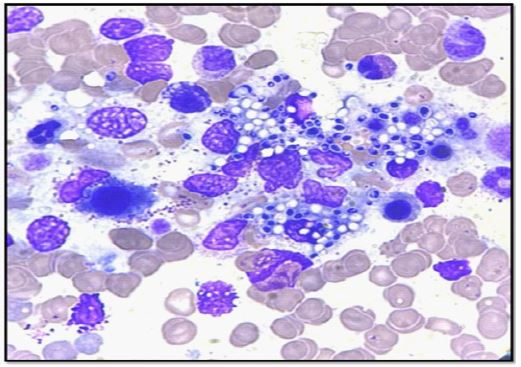
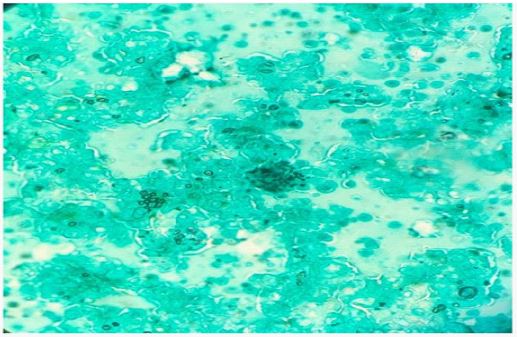
A 44 years old, North Indian male presented with complains of Rash, gum bleeding, epistaxis for 2 days. Medical history included known case of Type 2 Diabetes Mellitus, Hypertension, renal allograft recipient (donor-mother) in 2022 and mild COVID-19 disease in March 2023 managed at home. Bleeding manifestation was not associated with history of trauma, deep subcutaneous tissue and large joint bleeding, fever, weight loss, decrease appetite, cough and breathlessness. At the time of admission upon general examination patient appear normal built and height, well, nourished, temperature 37.5°F, Blood pressure -130/74 mmHg, pulse rate 100/min, Spo2-98% room air, Per abdomen examination revealed moderate splenomegaly, cardiovascular system and nervous system examination was with in normal limit. Head, ear, eyes examination was unremarkable except presence clot in nose, there was no lymphadenopathy. Initial medical report was Hemoglobin-6.8 g/dl, total leuckocyte count -3150 microL, Neutrophil -73%, Lymphocyte-13%, Eosinophil-02%, Monocyte-10%, Platelet count -1000/microL, Baseline Serum creatinine-1.8 mg/dl, Liver function test was normal. To rule out infectious causes of thrombocytopenia serologic test for HIV, Hepatitis B, Hepatitis C, scrub typhus IgM, leptospira IgM was sent which came out negative and dengue IgG was positive. Repeat Covid-19 test was also sent which was negative. Two sets of blood culture were also negative. Peripheral Blood Smear shows normocytic normochromic red blood cells, schistocyte index < 1.0%, WBC shows leucopenia with lymphopenia, Giant platelet was present with IPF of 2.5%. To rule out drug toxicity Serum Tacrolimus level was also sent which was 4.47 ng/ml, Serum ferritin was 3820 ng/ml, transferring saturation 43.55%, Vitamin B12-433 pg/ml, Serum LDH-157IU, Serum triglycerides-165 mg/dl. USG Doppler of transplanted kidney shows satisfactory perfusion. Despite all above test cause of severe thrombocytopenia remain uncertain. Supportive treatment to the patient given in form of 2 units single donor platelets transfusion, but platelets counts remain 1000/ μL. Later bone marrow aspiration was done and biopsy taken which showed high burden with histoplasma capsultum (Figure 1), confirmed with gomori methenamine stain for fungus (Figure 2) and a positive histoplasma urine antigen test further supported the diagnosis. He was started on injection amphotericin B with plan to transitioned to long course of itraconazole.
Discussion
Histoplasma capsulatum was first described by Samuel Darling in 1906. The fact that the organism looked like an encapsulated parasite inside a histiocyte prompted the name. The fungus is distributed worldwide, but endemic in certain areas of North and South America. In the United States, histoplasmosis is known to affect up to 90% of the residents of the Mississippi and Ohio River valleys. The means of patient exposure include contact with chicken houses, cutting down trees that have been known to be bird roosts, and spelunking in caves known to have large bat populations. Bird and bat excrement enhances the growth of the organism in soil by accelerating sporulation [1]. Clinical spectrum ranges from asymptomatic infection to life threatening illness in immunocompetent host Acute heavy exposure leads to flu like illness. Chest radiograph shows signs of pneumonitis with prominent hilar and mediastinal adenopathy. Disseminated histoplasmosis account for 70% of cases, common risk factors are AIDS (CD4 T cell count < 200/microliter, extreme age, Immunosuppressive medication and organ transplant most common with kidney transplant and maximum cases occur within 1 year of transplant (CID-4). Symptoms ranges from an acute, rapidly fatal course with diffuse interstitial or reticulonodular lung infiltrates causing respiratory failure, shock, coagulopathy, multiorgan failure to subacute or chronic course with a focal organ distribution with common features of fever, weight loss, hepatosplenomegaly and thrombocytopenia. Fungal culture remains the gold standard diagnostic test for histoplasmosis. However, culture results may not be known for up to 1 month, cultures are often negative in less severe cases. Cultures are positive in ~75% of patients with disseminated histoplasmosis and chronic pulmonary histoplasmosis. The detection of histoplasma antigen in body fluids is extremely useful in the diagnosis of DH and acute diffuse pulmonary histoplasmosis. The sensitivity of this method is >95% in patients with PDH and >80% in patients with severe acute pulmonary histoplasmosis resulting from heavy exposure, if both urine and serum are tested. Antigen levels correlate with severity of illness in PDH and can be used to follow the progression and treatment response. In biopsy specimen like Bone marrow or tissue biopsy yeast can be seen within circulating phagocytes on smears. Overall, bone marrow examination has the highest yield of isolating H. Capsulatum [1].
Similarly in our case risk factors of DH was Kidney transplant, and calcinurin inhibitor tacrolimus as immunosuppressive medication, and recent mild Covid infection. DH cases incidence are highest with post kidney transplant among all solid organ transplant patient and also calcinurin inhibitor is most common group drugs that associated with DH [2]. Donor derived histoplasmosis is rare. Case series published recently of 5 renal transplant also strengthen our finding that DH must be suspected in post renal transplant patient with pancytopenia [3].
Similar in our patient finding were similar like case series published of 5 patient post renal transplant pancytopenia with moderate splenomegaly as presentation with unusual manifestation of petechial rashes and epistaxis and gum bleeding due to severe thrombocytopenia. Several case reports have evaluated thrombocytopenia and histoplasmosis, and also interestingly thrombocytopenia in our patient did not responded to IV corticosteroids and IVIG similar to finding in case report [4]. Differential diagnosis in our case were drug induced pancytopenia, Miliary tuberculosis, disseminated cryptococcosis, Acute ITP, acute leukemia, Lymphoma. Several mechanism has been postulated to explain severe thrombocytopenia resulting from histoplasmosis infection, First is infiltration of bone marrow that may lead to impaired production. Second in human plasma H. Capsulatum can form a complex with IgG and fibrinogen and promote platelet aggregation and serotonin release. Third histoplasmosis may induce ITP and finally with disseminated infection, abnormal activation of coagulation system that leads to DIC and consumption of platelets [4]. In our patient initially we managed bleeding and severe thrombocytopenia with supportive platelet apheresis transfusion that patient not responded well, his platelet count remain low (1000/μL) despite 3 unit SDP (single donor platelet) transfusion, which could be explained by rapid destruction of platelets post transfusion as early as 2 hours post transfusion by autoimmune mechanism, and this autoimmune mechanism did not resolve until antifungal therapy instituted, similar to finding of kutkut et al. who suggested possible same [4].
Conclusion
Post renal transplant thrombocytopenia is a common blood disorder, persistent thrombocytopenia needs evaluation and management according to appropriate cause. As post organ transplant is a condition of immunosuppressed state, needs diagnostic workup for the causes that are less common in normal individual.
Declarations
Patient consent: The authors certify that they have obtained all appropriate patient consent forms. In the form, the patient has given his consent for giving clinical information to be reported in journal. The patients understand that their name and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
References
- Samannodi M, Minshawi F, Hasbun R. Disseminated histoplasmosis in a renal transplantation recipient: Peripheral blood smear was the key. Medical Mycology Case Reports. 2021: 30-1.
- Assi M, Martin S, Wheat LJ, Hage C, Freifeld A, Avery R, et al. Histoplasmosis after solid organ transplant. Clinical infectious diseases. 2013:1542-9.
- Rana A, Kotton CN, Mahapatra A, Nandwani A, Sethi S, Bansal SB. Post kidney transplant histoplasmosis: An under‐recognized diagnosis in India. Transplant Infectious Disease. 2021: e13523.
- Kutkut I, Vater L, Goldman M, Czader M, Swenberg J, Fulkerson Z, et al. Thrombocytopenia and disseminated histoplasmosis in immunocompetent adults. Clinical Case Reports. 2017: 1954.