
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Case report on aggressive central giant cell granuloma of mandible
Heena Yadav*; Hari Ram; Ravi Katrolia; Kipa Guma; Rangeet Bhadra
Department of Oral and Maxillofacial Surgery, Faculty of Dental Sciences, King George’s Medical University, Lucknow, UP, India.
*Corresponding Author : Heena Yadav
Junior Resident, Department of Oral and Maxillofacial Surgery, Faculty of Dental Sciences, King George’s Medical University, Lucknow, UP, India.
Email: ydvheena217@gmail.com
Received : Sep 09, 2023
Accepted : Sep 27, 2023
Published : Oct 04, 2023
Archived : www.jcimcr.org
Copyright : © Yadav H (2023).
Abstract
Central giant cell granuloma (CGCG) is an uncommon, benign but aggressive osteolytic neoplasm of the craniomaxillofacial region, histologically characterized by an abundance of evenly distributed multinucleated giant cells within a sea of spindle-shaped mesenchymal stromal cells, scattered throughout the fibrovascular connective tissue stroma containing areas of hemorrhage. A rapid diagnostic assessment, together with an adequate histopathologic verification, is essential to improve the management and the prognosis of this locally destructive lesion. A rare case of a large destructive CGCG involving the entire right side of mandible, causing extensive bony resorption, and buccal, medial as well as inferior border cortical expansion, in a young female is presented. It was treated successfully by surgical excision under general anesthesia.
Citation: Yadav H, Ram H, Katrolia R, Guma K, Bhadra R. Case report on aggressive central giant cell granuloma of mandible. J Clin Images Med Case Rep. 2023; 4(10): 2627.
Introduction
CGCG accounts for 7% maxillary tumors, and predominantly affect women in 2/3 of cases below 20 years of age group [1]. Aetiology of the lesion is idiopathic or unknown. It is postulated that it can arise as a result of factors such as inflammation, trauma, haemorrhage in the bone or genetic predisposition [2]. There are usually two types: The aggressive type and the non-aggressive types [3]. Surgical intervention is the considered the best over conservative approaches. Small lesions are removed by surgical curettage while larger lesions are removed by surgical resections [4].
Case presentation
A thirty one year old adult female patient reported to our department with swelling over the right lower jaw region since one and half years. The swelling was initially noted as pea-sized growth on right ramus region of mandible, which later progressed rapidly in size, to involve the entire right side of mandible (Figure 1). There was history of pain from the swelling reregion. No history of any trauma was given by the patient nor any systemic or local infections.
There was no history of similar diseases in any of the siblings or the parents of the affected female.
A physical examination revealed an adult female, who was not in any distress at presentation, with vital signs all within the normal range. The medical, drug and social history were not contributory. There was obvious facial deformity characterized by a diffuse swelling measuring approximately 10x8 cm in size extending supero-inferiorly from right angle region of mandible till infratemporal region and antero-posteriorly from mid of ala tragus line till right tragus region of face. The swelling was bony hard, with no tenderness and the overlying skin was of normal color and texture. The submandibular lymph nodes were enlarged measuring about 1.5x1.5 cm bilaterally but were freely mobile. Intra-orally mouth opening was adequate and all permanent teeth were present. There was a bucco-lingual expansion of the right posterior region of mandible with overlying mucosa appearing clinically healthy. The swelling had a consistency similar to bone and yielded no aspirate on aspiration. A clinical diagnosis of Ameloblastoma of mandible was made.
OPG showed a unilocular radiolucency, extending from right ramus region of mandible involving till subcondylar, coronoid process and infratemporal region. There was present pronounced cortical expansion and cortical thinning along the entire right ramus region of mandible. The lesion was not in close approximation with any teeth.

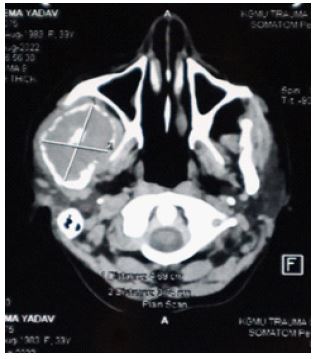
CECT (Figure 2) scan reports were suggestive of a well-defined heterogeneously enhancing osteoexpansile and osteolytic lesion measuring approximately 47x37x68 mm was noted in right infra-temporal fossa involving ramus, coronoid process and neck of condylar process of mandible involving right masseteric space. It was causing expansion of both outer and inner cortex with areas of cortical breach. The lesion was infiltrating the right masseter, right temporalis. Medially the lesion was abutting right lateral, medial pterygoid muscles with maintained fat planes. Posteriorly the lesion was abutting parotid gland with maintained fat planes. Antero-medially the lesion was abutting the posterior wall of maxilla, however no evidence of any bony erosion was seen. Few subcentimetric bilateral cervical lymph nnodes were noted, largest measuring approximately 16x7.7 mm in right level II.
Surgical excision of the lesion was done under general anesthesia. The lesion when exposed, had a soft spongy texture and appeared reddish-brown in colour interspersed with soft haemorrhagic areas that welled up with blood. The patient was followed up for a year, and no recurrence was noted (Figure 3). There was improves aesthetic appearance of the patient on follow up (refer to Figure 4).


Discussion
Correct diagnosis of bone tumours of the maxillofacial region can be quite challenging process. Numerous tumours present with similar clinical and radiological picture. The case report in our study had a short course of development hence it is an aggressive lsion which has caused obvious facial asymmetry. Aggressive pathological type of CGCG is characterized by rapid growth, root resorption, pain and even paresthesia in some cases [5]. Mainstay treatment being surgery was done for this case. The lesion was removed in toto and curettage was not needed to remove the further tumour remnants [6]. Surgical resection was not done as this was not a recurrent case and the inferior border of mandible was more than 1 cm thick [7]. Additionally, combination of cryosurgery and peripheral ostectomy reduces the rates of recurrence. Low recurrence rate has been reported with en bloc resection with a 5-mm margin [8]. In our case surgical excision is done with peripheral ostectomy. The defect was allowed to heal by primary intention.
Conclusion
Central Giant Cell Granuloma aggressive form can cause bony expansion thereby leading to aesthetic deformities as well as functional impairments. It is thus important to remove such lesions with adequate safety margin to prevent any sort of recurrence. Though various treatment modality exists for the management of CGCG it must be tailored according to age sex and socio-economic factors.
References
- Stage D, Pusel J, Janser JC, Rodier D, Philippe E. Lésions à cellules géantes de la mandibule: problèmes de diagnostic différentiel. A propos de trois cas de granulome central de réparation. In Annales d’oto-laryngologie et de chirurgie cervico-faciale. 1986; 103(3): 159-166.
- Lin YJ, Chen HS, Chen HR, Wang WC, Chen YK, Lin LM. Central giant cell granuloma of the mandible in a 7-year-old boy: a case report. Quintessence International. 2007; 38(3).
- Chuong R, Kaban LB, Kozakewich H, Perez-Atayde A. Central giant cell lesions of the jaws: a clinicopathologic study. Journal of oral and maxillofacial surgery. 1986; 44(9): 708-13.
- Eisenbud L, Stern M, Rothberg M, Sachs SA. Central giant cell granuloma of the jaws: experiences in the management of thirty-seven cases. Journal of oral and maxillofacial surgery. 1988; 46(5): 376-84.
- Haque AU, Moatasim A. Giant cell tumor of bone: a neoplasm or a reactive condition?. International journal of clinical and experimental pathology. 2008; 1(6): 489.
- Lin YJ, Chen HS, Chen HR, Wang WC, Chen YK, Lin LM. Central giant cell granuloma of the mandible in a 7-year-old boy: a case report. Quintessence International. 2007; 38(3).
- Gouin F, Grimaud E, Redini F, Moreau A, Passuti N, Heymann D. Metatarsal giant cell tumors and giant cell reparative granuloma are similar entities. Clinical Orthopaedics and Related Research (1976-2007). 2003; 416: 278-84.
- Inchingolo F, Tatullo M, Abenavoli FM, Marrelli M, Inchingolo AD, Inchingolo AM, Dipalma G. Non-Hodgkin lymphoma affecting the tongue: unusual intra-oral location. Head & neck oncology. 2011; 3(1): 1-5.