
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
A large retroperitoneal mass in a elderly male: A case report
Yelamanchi Hanock Devadoss1*; Gurmeet Singh Sarla2; Arnab Sengupta3; Mahesh Muraleedharan4
1Assistant Professor, Department of Surgery, Military Hospital Ahmednagar, Maharashtra, India.
2Senior Advisor Surgery, Military Hospital Khadki, Pune, Maharashtra, India.
3Assistant Professor, Department of Pathology, Military Hospital Ahmednagar, Maharashtra, India.
4Assistant Professor, Department of Radiology, Military Hospital Ahmednagar, Maharashtra, India.
*Corresponding Author : Devadoss YH
Assistant Professor, Department of Surgery, Military Hospital Ahmednagar, Maharashtra, India.
Tel: 91-8700809654
Email: edward.yelamanchi@gmail.com
Received : Sep 08, 2023
Accepted : Sep 28, 2023
Published : Oct 05, 2023
Archived : www.jcimcr.org
Copyright : © Devadoss YH (2023).
Abstract
Pain abdomen and distention of abdomen in elderly male, which is chronic in nature, draws attention to multiple differential diagnoses, especially if the individual has multiple comorbidities in the form of Systemic Hypertention, dyslipidemia. Ruling out aortic, renal, and gut pathologies clinically, biochemically and radiologically, the suspicion increases towards the intra-abdominal pathology [1]. The patient initially had swelling in left hypochondriac area which gradually increased over a period of 12 years and extended towards both lumbar regions and right iliac fossa associated with dull aching pain around left hypochondriac area [2]. Patient denied history of previous abdominal surgeries. Surgical removal is treatment of choice for a symptomatic patient with retroperitoneal mass. However, the controversy surrounding the surgical removal goes with histopathological outcome of the specimen [3]. As a norm the retroperitoneal tumors are slow growing and the chances of malignant transformation increases with size and duration, high suspicion of sarcomatous transformational pathology should be kept in mind [4].
Keywords: Abdominal mass; Lipoma; Retroperitoneum.
Citation: Devadoss YH, Sarla GS, Sengupta A, Muraleedh M. A large retroperitoneal mass in a elderly male: A case report. J Clin Images Med Case Rep. 2023; 4(10): 2630.
Introduction
Lipomas are exceedingly rare in the retroperitoneum, and this diagnosis should be made with caution because most lesions designated as retroperitoneal lipoma are lipoma like areas of an under sampled, well-differentiated liposarcoma. It is generally understood that the deeper and more centrally located a fatty mass resides, the more likely it is to be malignant [5].
Case report
70 year old retired gentleman presented with complaint of lump abdomen which gradually increased in size over 12 years occupying left hypochondrium, left lumbar, left ilac fossa, crossing midline below umbilicus with symptoms of lower GI tract involvement in the form of intermittent constipation. No history of mass or bleeding per rectum. No history of hematuria. No history of anorexia, weight loss, generialised malaise, fever. No history of TYPEIIDM, hypertention, TB, epilepsy. No history of previous hospital admissions or abdominal surgeries for the same.
On examination GC fair ECOG status-1, Pulse: 84 Per min, Blood pressure: 142/90 mm of hg, Spo2: 99% on room air, no pallor icterus, cyanosis, clubbing pedal edema, lymphadenopathy. Per Abdomen examination: soft lobulated mass 25 cm craniocaudally, 10 cm from umbilicus medially, 10 cm from mid axillary line laterally extending from left hypochondrium, left lumbar, crossing midline towards right iliac fossa below umbilicus, not moving with respiration, but ballotable, fingers could not be insunated below the superior, inferior, mediolateral margins. On digital rectal examination: stool stain over gloved finger, no mass palpable, on proctoscopy no mass or hemorroids visualized.
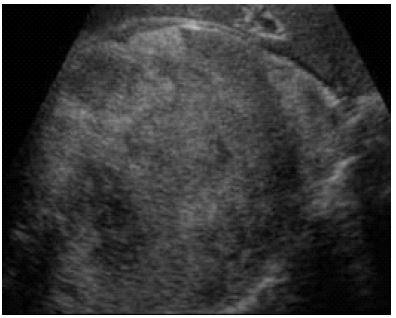
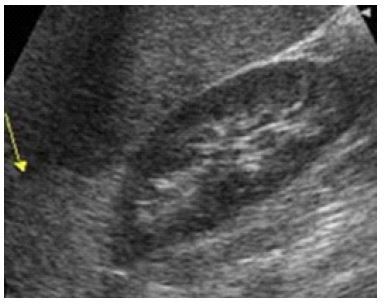
On evaluation total leucocyte count was 6500 cells/cu.mm, Neutrophils: 65%, Lymphocytes: 24%, eosiniphils: 10%, monocytes: 1%, basophils: nil. SGOT/SGPT: 28/32 IU/L, ultrasonography of abdomen suggestive of large fat density of 36x22x8 cm in size, present in left half of abdomen, displacing small bowel loops to right side, lesion abutting the left lower pole kidney with clear margin not breaching gerotas fascia. Contrast Enhanced Compted Tomography of abdomen suggestive of large fat density of 40x25x8 cm in size oval well defined lesion present in left half of abdomen, displacing small bowel loops to right side, lesion showing thin impercitible wall and abutting the left gerotas fascia, represent retroperitoneal lipoma to be correlated histopathologically.


Patient underwent exploratory laparotomy with excision of lesion with epidural analgesia Under general anaethesia, per operatively 42x28x10.5 cm lipomatous lesion arising from retroperitoneum, displacing the left paracolic gutter, peritoneum left ureter, bowel loops to right. Abdominal drain removed on post op day 05, and patient was discharged and was followed by contrast enhanced tomography of abdomen after 03, 06 months with no evidence of recurrence till date.




Discussion
Giant retroperitoneal lipomas in adults are scarce, with a total number of 17 cases described in the literature since 1980. Subcutaneous lipomas are associated with hypercholesterolemia, obesity and trauma, whereas such data does not exist for retroperitoneal lipomas [6]. Moreover, the patient was not described positive for any of these factors. Retroperitoneal lipomas are usually asymptomatic for a long time before they cause abdominal swelling or symptoms due to obstruction or shifting of adjacent organs and structures [7]. At this point, they may have already reached enormous size. This may be explained by the great retro-peritoneal space that allows them to grow before they get symptomatic and the slowness of their enlargement [8].
The diagnosis is based on a MRI (magnetic resonance imaging) or CT-scan, yet both imaging modalities may not exclude a well-differentiated liposarcoma. Furthermore, biopsies often remain inconclusive. The incidence of soft-tissue sarcomas in general is described with 4 cases per 100.000 and year of which liposarcomas are the most common and are located in one third of cases in the retroperitoneum [9].
The incidence of retroperitoneal lipomas on the other hand is thought to be extremely rare. Hence, a well-differentiated liposarcoma may not be ruled out preoperatively, even if a benign lipoma is clinically suspected. Therefore, intraoperative judgment about tumor characteristics and subsequent decision making about the extent of resection is of great importance. R0 Resection is mandate in every case [10].
Primary retroperitoneal tumors are rare and have great histological variety. They may originate from the retroperitoneal adipose, muscle, connective, lymphatic and nerve tissue, and from the urogenital tract [11]. Malignant primary retroperitoneal tumors represent less than 1% of all neoplasms diagnosed.Although soft-tissue sarcomas are more common among adults, retroperitoneal liposarcomas represent only 0.1% to 0.2% of all malignant neoplasms [12].
Sole extirpation should be reserved for clearly circumscribed tumors. However, due to the enormous size of the tumor preoperative judgment about resectability based on CT-scans is difficult [13]. Therefore, tumor debulking for symptom relief can also be discussed if oncological resection is not feasible [14].
Due to the possible malignant nature of such retroperitoneal tumors resection should be carried out by a trained oncological surgeon in a center of excellence for soft-tissue sarcomas [14].
Eresure et al. described two cases with dimensions of 15x 40 and 13x18 cm, respectively, and attributed the size of the tumors to their characteristics of slow and progressive growth [15].
In this patient of the present report, the same characteristics were also observed, that the lesion had large dimensions (42x28x10.5 cm) and weighed 8.45 kg. In this case the tumor was clearly demarcated macroscopically and without any sign of infiltrative growth [16,17] all though, the enormous size was present but no infilterative margins allowed accomplishing an oncological correct resection [18,19]. Since clinical and ex-perimental data on tumor progression and tumor recurrence of retroperitoneal lipomas are lacking a close and regular follow-up is indicated.
Conclusion
Presence of large retroperitoneal lipomas are rare and careful evaluation of histopathology is mandated in every case to rule out sarcomatous lesion, nevertheless the tumour clearance should be considered respecting oncological principles [20]. In this case the whole lesion was lipomatous with no high grade or sarcomatous change involvement.
Conflict of interest: There is no conflict of interest to declare by any of the authors of this study.
References
- Bengmark S, Hafstrom L, Jonsson PE, Karp W, Nordgren H. Retroperitoneal sarcomas treated by surgery. J Surg Oncol 1980; 14: 307-14.
- Jensen Benítez C, Vergara Bahamondes JI, Aparicio R, Ibarra A, Chomali T. Tumores primaries retroperitonealesde origemmesenquimático. Rev Hosp Clin Univ Chile 1994; 5:58-64.Usandivaras JR, Díaz San Román AH. Resección de tumors retroperitoneales. Rev Med Tucuman. 2001; 7: 23-32.
- Marshall MT, Rosem P, Berlin R, Gresson N. Appendicitis masquerading as tumor: a case of two diagnoses. J Emerg Med 2001; 21: 397-9.
- Shouzhu Z, Xinhua Y, Xumin L, Shulian L, Xianzhi W. Giant retroperitoneal pleomorphic lipoma. Am J SurgPathol 1987; 11: 557-62.
- Zhang SZ, Yue XH, Liu XM, Lo SL, Wang XZ. Giant retroperitoneal pleomorphic lipoma. Am J SurgPathol 1987; 11: 557-62.
- Marshall MT, Rosen P, Berlin R, Greenson N. Appendicitis masquerading as tumor: a case of two diagnoses. J Emerg Med. 2001; 21(4): 397-9.
- Matsubara N, Yoshitaka T, Matsuno T, Ikeda M, sozaki, Tanaka N, et al. Multiple tumors and a novel E2F-4 mutation. A case report. Digestion. 2000; 62(2–3): 213-6.
- Acheson A, McIlrath E, Barros D’Sa AA. Pelvic lipoma causing venous obstruction syndrome. Eur J Vasc Endovasc Surg. 1997; 14(2): 149-50.
- Zhang SZ, Yue XH, Liu XM, Lo SL, Wang XZ. Giant retroperitoneal pleomorphic lipoma. Am J Surg Pathol. 1987; 11(7): 557-62.
- Deppe G, Malviya VK, Hercule J, Gleicher N. Retroperitoneal pelvic lipoma. J Natl Med Assoc. 1985; 77(7): 574-6.
- Rubinstein A, Goor Y, Gazit E, Cabili S. Non-symmetric subcutaneous lipomatosis associated with familial combined hyperlipidaemia. Br J Dermatol. 1989; 120(5): 689-94.
- Self TH, Akins D. Dramatic reduction in lipoma associated with statin therapy. J Am Acad Dermatol. 2008; 58(2 Suppl): S30-1. doi:10.1016/j.jaad.2007.08.034.
- da Pires Botelho Costa JS, Reis JC, Valenca-Filipe R, et al. Giant atypical lipoma of the thigh. Dermatol Surg. 2014;40(2):213–4. doi:10.1111/dsu.12397.
- Van Thielen J, Van Loo S, Van der Stighelen Y. Case report: a gastric lipoma in a morbid obese man. Acta Chir Belg. 2012; 112(5): 393-4.
- Zografos GC, Kouerinis I, Kalliopi P, Karmen K, Evagelos M, Androulakis G. Giant lipoma of the thigh in a patient with morbid obesity. Plast Reconstr Surg. 2002; 109(4): 1467-8.
- Aust MC, Spies M, Kall S, Jokuszies A, Gohritz A, Vogt P. Posttraumatic lipoma: fact or fiction? Skinmed. 2007; 6(6): 266-70.
- Leffell DJ, Braverman IM. Familial multiple lipomatosis. Report of a case and a review of the literature. J Am Acad Dermatol. 1986; 15(2 Pt 1): 275-9.
- Casali PG, Jost L, Sleijfer S, Verweij J, Blay JY. Soft tissue sarcomas: ESMO clinical recommendations for diagnosis, treatment and follow-up. Ann Oncol. 2008; 19 Suppl 2:ii 89-93. doi:10.1093/annonc/mdn101.
- Dalal KM, Antonescu CR, Singer S. Diagnosis and management of lipomatous tumors. J Surg Oncol. 2008; 97(4): 298-313. doi:10.1002/jso.20975.
- Soft tissue and visceral sarcomas: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2012; 23 Suppl 7: vii92-9. doi:10.1093/annonc/mds253.