
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Paediatric thoracic actinomycosis presenting as back swelling: A case report
Deirdre Foley1*; Claire Connellan2; Fiona Healy2; Patrick Gavin1
1Department of Infectious disease and Immunology, Children Health Ireland Crumlin and Temple Street hospitals, Dublin, Ireland.
2Department of Respiratory Medicine, Children Health Ireland Crumlin at Temple Street, Dublin, Ireland.
*Corresponding Author : Deirdre Foley
Department of Infectious Disease and Immunology, Children’s Health Ireland at Crumlin, Ireland.
Email: Deirdrefoley731@gmail.com
Received : Sep 14, 2023
Accepted : Oct 03, 2023
Published : Oct 10, 2023
Archived : www.jcimcr.org
Copyright : © Foley D (2023).
Abstract
Presentation: A seven years old girl presented with a three-day history of cough and fever, and several weeks of back pain, anorexia and weight loss. Examination was significant only for a tender, non-erythematous swelling to the right mid-back measuring ten centimetres in length.
Diagnosis and treatment: Investigations on admission included neutrophilia and elevated inflammatory markers. Chest radiograph demonstrated a confluent area of opacification within the right peripheral lower zone with a small pleural effusion. CT reported two large enhancing and infiltrative lesions in the right thorax and the right posterior lower ribs, and disseminated lymphadenopathy. Microbiology and histology of a tissue sample were conclusive for actinomycosis israelii. She had a full recovery following a nine month course of oral amoxicillin.
Discussion: Invasive actinomycosis is rare, and a high clinical suspicion and thorough investigation is warranted with invasive pneumonia and atypical associated symptoms.
Keywords: Actinomycosis; Pneumonia; Chest wall mass; non-accidental injury.
Abbreviations: ASD: Autism Spectrum Disorder; CMV: Cytomegalovirus; CRP: C-Reactive Protein; EBV: Epstein Barr Virus; ESR: Erythrocyte Sedimentation Rate; HIV: Human Immunodeficiency Virus.
Citation: Foley D, Connellan C, Healy F, Gavin P. Paediatric thoracic actinomycosis presenting as back swelling: A case report. J Clin Images Med Case Rep. 2023; 4(10): 2635.
Introduction
Actinomycosis is an uncommon, invasive and slowly progressive infection in children. These gram-positive bacteria are facultative anaerobes and live as part of the normal human flora. Thoracic disease accounts for [14 ]. To 34% of paediatric actinomycosis cases [1]. There is a higher incidence of thoracic actinomycosis in adults than children, and in males than females. Incidence rates of actinomycosis of 1 in 300,000 persons have been reported, but this has reduced in line with improved healthcare and dental hygiene [2]. Overall, paediatric actinomycosis is rare, accounting for less than 3% of all actinomycosis case. Risk factors for infection include poorly controlled diabetes mellitus, trauma and dental caries.
Case report
A seven years-old female, presented to our emergency department with a tender mass to the right mid-back and a three-week history of intermittent cough and fever, anorexia, back pain and weight loss in the month prior to presentation. She had received a short course of oral amoxicillin early in the course of this illness, which resulted in a brief improvement of her symptoms. She alleged that she was struck with a stick to the area by an adult six-days prior to presentation, and was assessed by her general practitioner and referred to the emergency department due to concern of non-accidental injury.
Background medical history was significant only for well-controlled asthma and autism spectrum disorder. She was of Southern African ethnicity but born in Ireland and up to date with the full primary immunisation schedule. Her parents reported that her brother had passed away at the age of three years from a ‘neck lump’, with his final diagnosis unclear. There was no significant family history of retrovirus or mycobacterial exposures, and her last travel to Sub-Saharan Africa was two years ago.
On examination she had a tender, non-erythematous, non-fluctuant swelling to the right mid-back, measuring 10 cm in length and 3 cm in diameter. Respiratory examination noted good air entry bilaterally. There was no evidence of lymphadenopathy, rash or joint involvement, and she required no additional oxygen or respiratory support.
Investigations were significant for an elevated CRP [126 mg/L], Erythrocyte Sedimentation Rate of 83 [mm/H], white cell count of 16.3x109 /L and neutrophils of 10.9x109/L. Chest radiograph demonstrated a confluent area of opacification within the right peripheral lower zone and a small pleural effusion. She was commenced on intravenous amoxicillin as treatment for suspected community acquired pneumonia.
During admission, ultrasound of her left lower chest wall reported a solid lesion in appearance with some colour doppler flow between the right lower posterior ribs. Contrast computed tomography [CT]. Identified a multi-focal abnormality with two discontinuous enhancing and infiltrative lesions. The first lesion was a pleural based mass with extension to the right heart border and right thorax [5x2.9x3.9 cm]. The second lesion was centred around the right posterior lower ribs [7.4x3.4x9.4 cm] with mass effect on the right kidney and extending into the paraspinal soft tissue, posterior renal space and local musculature. There was mild periosteal reaction in the adjacent ribs but no bony erosion, and mediastinal, right hilar and right axillary lymphadenopathy was present.

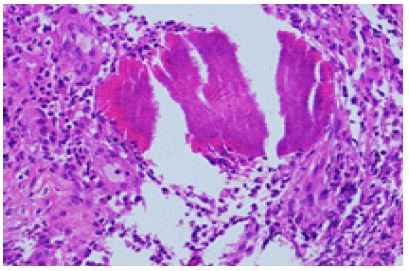
Infectious disease screen included a negative Mantoux, QuantiFERON, Human Immuno-deficiency Virus [HIV] Antibody, Epstein-Barr Virus [EBV] and Cytomegalovirus [CMV] Serology. Immunology work-up demonstrated a low IgM 0.4 [0.5-1.8 g/L] But normal IgG and IgA. Vaccine specific pneumococcal titres were low in nine serotypes, for which she received a booster with the 13-valent pneumococcal polysaccharide conjugate vaccine. Mycobacterial culture and 16S polymerase chain reaction [PCR] were negative. Histological staining demonstrated a fibro-inflammatory process, with necro-inflammatory debris containing sulphur granules consistent with actinomyces. Chest wall tissue culture was positive for a scanty growth of Actinomyces Israelii.
Administration of penicillin-based antibiotics resulted in a rapid improvement in energy, appetite, and the back swelling quickly resolved over the course of four days. Inpatient dental review identified severe decay in a left lower molar suggestive of chronic infection, but no associated soft tissue inflammation or discharging sinus. Elective dental extraction was performed several weeks later. She was discharged home on high dose oral amoxicillin after a ten-day inpatient stay. The total duration of anti-biotic therapy was nine months, at which point compliance had significantly deteriorated. Imaging had normalised by twelve weeks of therapy and ultrasound and chest radiograph 11 months after diagnosis remained unremarkable.
Discussion
In this case we report an unusual presentation of a rare infection in a well child. The unusual illness her sibling had passed away from raised concern of an inherited predisposition to malignancy, mycobacterial infection or other atypical infection. Underlying immunosuppression from acquired or inherited immunodeficiency was also a differential. The diagnostic process was confounded by her initial reasons for referral to the emergency department-concern of the soft tissue injury from non-accidental injury. Utilising a conservative approach and thorough medical social work assessment, no child safe-guarding concerns were identified.
Oral amoxicillin has excellent bioavailability and is thought to be equally efficacious to phenoxymethylpenicillin, with the advantage of three times daily dosing [3,4]. Actinomyces species are uniformly susceptible to penicillin and rarely acquires resistance to penicillin antibiotics during prolonged therapy [5]. An early oral switch is possible, even in invasive disease, if susceptible. Traditional reports suggested that initial intravenous therapy is typically given for two to six weeks, followed by six to twelve months of oral antibiotic therapy for the treatment of thoracic actinomycosis. In some cases, a combined medical-surgery approach is necessary to manage complicated disease [2]. A retrospective review found excellent outcomes (96% cure and no clinical evidence of recurrence) with conservative management [6]. Though mortality from untreated actinomycosis can be high outcomes have been significantly improved, and the majority of cases of those with paediatric actinomycosis who receive appropriate and timely anti-microbial treatment have good clinical outcomes [7].
References
- Bartlett AH, Rivera AL, Krishnamurthy R, Baker CJ. Thoracic Actinomycosis in Children. Pediatric Infectious Disease Journal. 2008; 27(2):165-9.
- Okulicz JF, Polenakovik H, Polenakovik S. Actinomycosis [Internet]. Medscape. 2022; (18): Available from: https://emedicine.medscape.com/article/211587-overview#a6
- Martin M V. The use of oral amoxycillin for the treatment of actinomycosis. A clinical and in vitro study. Br Dent J. 1984; 156(7): 252-4.
- Arancibia A, Guttmann J, González G, González C. Absorption and disposition kinetics of amoxicillin in normal human subjects. Antimicrob Agents Chemother. 1980; 17(2): 199-202.
- Steininger C, Willinger B. Resistance patterns in clinical isolates of pathogenic Actinomyces species. Journal of Antimicrobial Chemotherapy. 2016; 71(2): 4227.
- Choi J, Koh WJ, Kim TS, Lee KS, Han J, Kim H, et al. Optimal Duration of IV and Oral Antibiotics in the Treatment of Thoracic Actinomycosis. Chest. 2005; 128(4): 2211-7.
- Bates M, Cruickshank G. Thoracic Actinomycosis. Thorax. 1957; 12(2): 99-124.