
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Imge - Open Access, Volume 4
Embolization and bleeding in patients with anticardiolipin antibodies
Fan Wei1,2; Wang Wenhui2*
1The First Clinical Medical College of Lanzhou University, China.
2Department of Interventional medicine, The First Hospital of Lanzhou University, China.
*Corresponding Author : Wang Wenhui
Department of Interventional Medicine, The First Hospital of Lanzhou University, Chengguan District, Lanzhou, Gansu, China.
Email: wangwenhui1968@126.com
Received : Sep 13, 2023
Accepted : Oct 05, 2023
Published : Oct 12, 2023
Archived : www.jcimcr.org
Copyright : © Wenhui W (2023).
Keywords: Anti-cardiolipin antibody syndrome; Hemoptysis; Bronchial artery embolization.
Citation: Wei F, Wenhui W. Embolization and bleeding in patients with anticardiolipin antibodies. J Clin Images Med Case Rep. 2023; 4(10): 2640.
Background
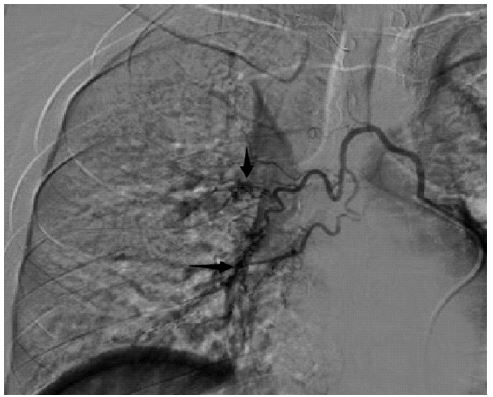
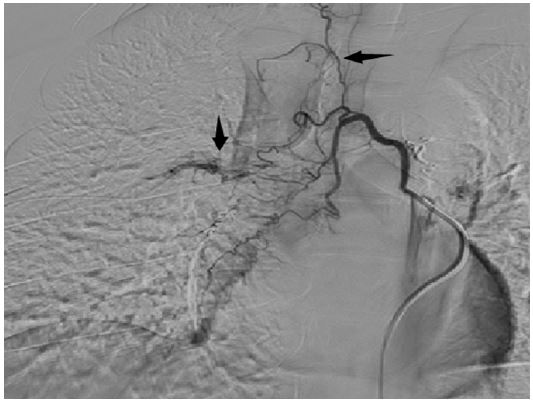
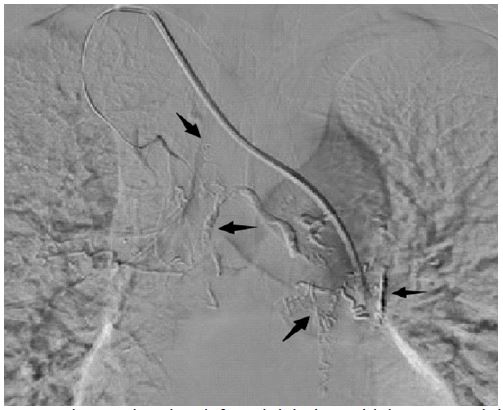
The patient, a 32-year-old male, was positive for anti-cardiolipin antibody syndrome and had a history of smoking for 15 years. He underwent “inferior vena cava filter implantation + catheter hemolysis” 10 years ago due to deep vein thrombosis of the right lower limb. After surgery, he continued to take farwarin and aspirin orally. Three years ago, due to thrombosis again, intravenous thrombolysis was performed in the lower extremity. After surgery, pharhualin was taken orally continuously. Massive hemoptysis occurred after intense exercise and eating spicy stimulating food 5 months ago. DSA showed abnormal bleeding in the right bronchial artery and right internal thoracic artery, so 300-500 um microsphere was used to embolize the peripheral artery. 350-560 um PVA granules embolized bronchial arteries; Three months ago, due to the recurrence of hemoptysis after oral administration of TCM blood-promoting drugs, angiography showed an increase in the number of responsible arteries, abnormal bleeding of the left bronchial artery and the right upper lobar bronchial artery of the lung segment, the formation of the middle and lower lobar bronchial artery of the right lung segment and the formation of collateral circulation of the right internal thoracic artery. Embolization of the above arteries was performed, and the patient recovered well after surgery and was discharged from hospital.



Discussion
The diagnosis of antiphospholipid antibody syndrome requires continuous elevation of laboratory indicators (lupus anticoagulant, anticardiolipin antibody IgG/IgM, or anti-β2 glycoprotein I antibody IgG/IgM) for more than 12 weeks and the presence of clinical symptoms (thrombus or miscarriage). The main clinical features of the disease are small and recurrent arteriovenous (more common) progressive thrombus. It usually occurs in young people between 20 and 40 years old [1], and the blood test mainly changes the Prothrombin Time (PT) and Activated Partial Thrombin Time (APTT), it can involve various organs, and the lungs are manifested as pulmonary embolism or pulmonary infarction, and the probability of hemoptysis is very small [2]. The probability of thrombocytopenia in this disease is about 20%, and the probability of upper respiratory tract infection is about 9% [3]. Smoking will aggravate lung infection and lead to bleeding. The possible reason is that oxidative stress of anti-phospholipid antibodies leads to high concentration of C-reactive protein and PGE2 and other inflammatory mediators. This patient has anti-cardiolipin antibody type, IgG and α-β2GP1 continuously elevated. Systematic treatment of APS includes antiplatelet therapy (low-dose aspirin, hydroxychloroquine) and long-term postoperative anticoagulant therapy with vitamin K antagonists [4,5]. In recent years, direct oral anticoagulants (rivaroxaban, dabigatrun) have also become an effective choice for the treatment of this disease [6]. However, for patients with acute hemoptysis, the treatment of this disease is more effective. Bronchial artery embolization remains the recommended option for symptom control.
References
- Al-Adhoubi NK, Bystrom J. Systemic lupus erythematosus and diffuse alveolar hemorrhage, etiology and novel treatment strategies. Lupus. 2020; 29: 355-363.
- Arreola-Diaz R, Majluf-Cruz A, Sanchez-Torres LE, Hernandez-Juarez J. The Pathophysiology of the Antiphospholipid Syndrome: A Perspective from the Blood Coagulation System. Clin Appl Thromb Hemost. 2022; 28: 10760296221088576.
- Bernardoff I, Picq A, Loiseau P, Foret T, Dufrost V, et al. Antiphospholipid antibodies and the risk of autoimmune hemolytic anemia in patients with systemic lupus erythematosus: A systematic review and meta-analysis. Autoimmun. Rev. 2022; 21: 102913.
- Devreese KMJ, Groot PG, Laat B, Erkan D, Favaloro EJ et al. Guidance from the Scientific and Standardization Committee for lupus anticoagulant/antiphospholipid antibodies of the International Society on Thrombosis and Haemostasis: Update of the guidelines for lupus anticoagulant detection and interpretation. J. Thromb. Haemost. 2020; 18: 2828-2839.
- Vandevelde A, Devreese KMJ. Laboratory Diagnosis of Antiphospholipid Syndrome: Insights and Hindrances. J Clin Med. 2022; 11: 2164.
- Petri M. Antiphospholipid syndrome. Transl Res. 2020; 225: 70-81.