
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Rombo encephalitis and cerebellar abscess due to Listeria monocytogenes with fulminant course in an immunocompetent elderly patient: A case report
Juan Francisco García Granado1*; Carmelo Monzón Moreno2; María del Pino Pérez García3; Juan Carlos López Fernández4
1Neurology Service of the University Hospital of Gran Canaria Doctor Negrín, Spain.
2ULPGC and Microbiology Service of the San Roque University Hospital, Spain.
3Gran Canaria Primary Care Department Laura López Delgado, University Hospital Complex Insular Materno Infantil, Infectious Diseases Service, Spain.
4Neurology Service San Roque University Hospital, Spain.
*Corresponding Author : Juan Francisco García Granado
Neurology Service, University Hospital of Gran Canaria Doctor Negrín, Las Palmas, Canary Islands, Spain.
Email: juuanfra21@gmail.com
Received : Sep 15, 2023
Accepted : Oct 06, 2023
Published : Oct 13, 2023
Archived : www.jcimcr.org
Copyright : © García Granado JF (2023).
Abstract
Listeria Monocytogenes (LM) is an opportunistic bacterium that can cause from mild infections to severe clinical pictures with neurological involvement, being responsible for sporadic cases, epidemic outbreaks and a high mortality and case fatality rate.
Neurolisteriosis may present as meningitis, meningoencephalitis, rhomboencephalitis or brain abscesses. LM rhomboencephalitis is a rare disease for which advanced age and cellular immunosuppression are common risk factors, although it may occur in patients without prior immunosuppression. Spread to the CNS occurs haematogenously through the blood-brain barrier, by direct invasion or by retrograde brain migration through nerve tracts. Different diagnostic subtyping methods are available, although DNA sequencing is the technique of choice for epidemiological studies. The combination of ampicillin with gentamicin for 6-8 weeks is usually the recommended treatment, and neurosurgery may improve the prognosis in patients with brain abscess, although there are no clinical practice guidelines available with a high level of evidence.
The diagnosis of LM rhomboencephalitis should be suspected in any patient with an infectious condition with evidence of meningeal or brainstem involvement. Mortality from neurolisteriosis is increasing in Europe due to the ageing population and the increase in immunocompromised patients, and can reach up to 51%. The case described in this article is exceptional, presenting acute rhomboencephalitis with cerebellar abscesses in a healthy patient with no risk factors and a fulminant course.
Keywords: Listeria monocytogenes; Rombo encephalitis; Cerebelar abscess.
Abbreviations: LM: Listeria Monocytogenes; CNS: Central Nervous System; DNA: Deoxyribonucleic Acid.
Citation: García Granado JF, Monzón Moreno C, Pérez García MDP, López Fernández JC. Rombo encephalitis and cerebellar abscess due to Listeria monocytogenes with fulminant course in an immunocompetent elderly patient: A case report. J Clin Images Med Case Rep. 2023; 4(10): 2641.
Introduction
Listeria monocytogenes (LM) is an intracellular, opportunistic, gram-positive, digestive-borne bacillus that can cause gastroenteritis to invasive clinical conditions with severe neurological involvement, bacteraemia and septic shock.
In Europe, a 31% increase in mortality from listeriosis was observed between 2018 and 2019, due to an ageing population and an increase in the number of immunocompromised patients. In 2018, the incidence in Spain was 0.89/100,000 inhabitants, with the most virulent serotype being ST87 [1]. An outbreak of LM subtype 4b/ST388 associated with the consumption of larded meat occurred in 2019 in Andalucia [2]. The case fatality rate in Europe reaches 17% when LM causes neurological involvement, being more frequent in people older than 65 years and with cellular immunosuppression [3]. Brain stem encephalitis occurs in only 17% of patients, but with a mortality of up to 51%, with a fulminant course in most patients [4].
LM can invade the CNS retrogradely via nerve tracts, by haematogenous spread from the gastrointestinal tract to the choroid plexus or even reach the brain parenchyma via the cerebral capillary endothelium [4]. The most common clinical manifestation is meningitis, which occurs in 20% of the elderly, while meningoencephalitis, rhomboencephalitis, cerebritis and brain abscesses are less frequent [4-5].
A mainstay of microbiological diagnosis is blood cultures, which have a diagnostic yield of 60%, although second-generation diagnostic sequencing has been able to detect pathogens in CSF from culture-negative patients, improving diagnostic efficiency and yield [5].
Case presentation
A 79-year-old man with a history of hypertension, hypercholesterolemia and ischaemic heart disease was admitted for a febrile syndrome of 38°C, impaired level of consciousness, gait instability and vertiginous syndrome of 5 days’ evolution with a normal initial brain Computed Tomography (CT) scan. On neurological examination, peripheral facial palsy and left palpebral ptosis, horizontal-rotatory nystagmus in all gaze directions and left appendicular dysmetria were documented.
The requested complementary analytical tests showed a leukocytosis of 15.38 x 103/uL (4.00-11.00 x 103/uL) with 4.6% (15.00-50.00%) of lymphocytes and 86.7% (45.00-75.00%) of neutrophils, a ferritin of 65.5 ng/ml (21.81-274.66 ng/ml), glucose of 140 mg/dl (70-100), creatinine of 1. 5 mg/dl (0.73-1.18 mg/dl), C-reactive protein (CRP) of 1.7 mg/dl (< 0.5), aspartate aminotransferase (AST) of 100 U/L, lactate dehydrogenase (LDH) of 410 U/L and free T4 of 2.9 ng/dl (0.7-1.48 ng/dl), with all other systematic biochemical and hormonal parameters within normal. Coagulation and tumour markers were normal except for the presence of an International Normalised Ratio (INR) of 1.12 and a D-dimer of 13447.5 ng/ml (<500 ng/ml). In addition, urine culture and urine culture and HIV-1/HIV-2 serology, antibodies and P24 antigen were negative.
The requested blood cultures showed Gram-positive bacilli, meeting microbiological criteria for isolation of penicillin- and ampicillin-sensitive Listeria monocytogenes. The cerebrospinal fluid extracted by lumbar puncture was clear and yellowish, without turbidity and with presence of xanthochromia, normoglycaemia, hyperproteinuria of 225 mg/dl (15-45 mg/dl) and a lactate of 7.1 mmol/L (< 2 mmol/L). Based on cerebrospinal fluid cytobiochemical results, cell counts were 20 red blood cells/μL and 1550 leukocytes/μL with 72% mononuclear and 28% polymorphonuclear. Listeria monocytogenes was finally isolated in the CSF culture.
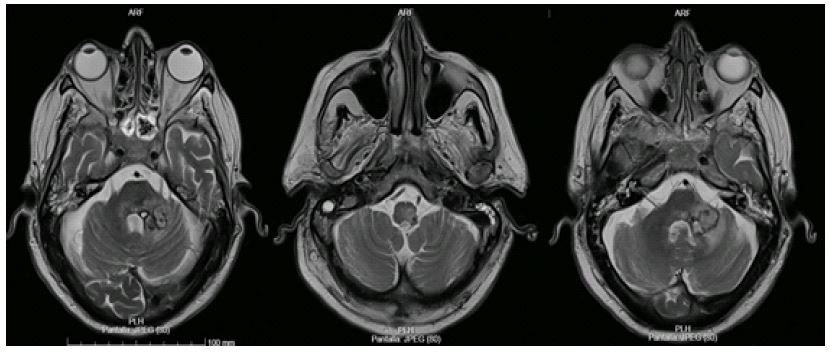
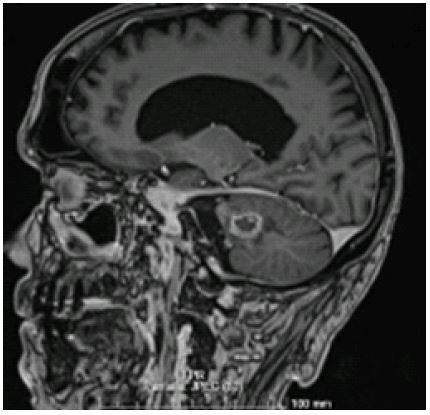
Magnetic Resonance Imaging (MRI) of the brain, performed at 24 hours, revealed a lesion in the left middle cerebellar peduncle with truncal-brain extension and to the left cerebellar hemisphere of heterogeneous appearance, polylobulated and with central and peripheral contrast uptake pattern, measuring approximately 2.5 x 2.2 cm in axial plane and with a small amount of perilesional vasogenic oedema. Communicating hydrocephalus was also observed (Figures 1,2).
The patient showed symptoms compatible with a meningeal syndrome with posterior cerebral topographic involvement in which the liquefaction profile, microbiological isolation by blood cultures and neuroradiological findings led to the conclusion that this was an infectious rhomboencephalitis due to Listeria monocytogenes associated with a cerebellar abscess.
He was treated empirically with gentamicin 600 mg/day, linezolid 600 mg/12 h, ampicillin and dexamethasone with subsequent de-escalation to ampicillin and cotrimoxazole due to the antibiogram findings, with little response and progressive neuroradiological, haemodynamic and general and neurological symptoms worsening. As the patient experienced a marked deterioration in respiratory mechanics and deterioration of the level of consciousness with signs of decerebration, it was decided to transfer him to the Intensive Care Unit (ICU) and intubate him (Cormack 1).
In a third control CT scan, associated with the lesions described, non-communicating hydrocephalus was observed in the context of an expansive lesion in the posterior territory that caused extrinsic pseudotumoural compression of the fourth ventricle, Therefore, an urgent External Ventricular Drainage (EVD) catheter was placed with monitoring of Intracranial Pressure (ICP) by means of right frontal trepanation and distal insertion of the catheter in the frontal horn of the ipsilateral lateral ventricle, with subsequent initiation of intrathecal antibiotic therapy with vancomycin.
Given the clinical-radiological worsening of the patient, persistent low level of consciousness with Glasgow Coma Scale (GCS) of 6 points (O2V1M3) and onset of Generalised Tonic-Clonic Seizures (CTCG), neurological sedation with propofol 200 mg/h with Richmond Agitation and Sedation Scale (RASS) of 4 points was performed.
The patient presented haemodynamic deterioration with a rising requirement for noradrenaline and the start of vasopressin, with deterioration of renal function. The patient also had a torpid evolution from the neurological point of view, with failure of antibiotic treatment. In addition, a cranial CT scan showed a slight amount of intraparenchymal haemorrhage, adjacent to the path of the shunt catheter, with an opening towards the ventricular system, located in the declivity of both occipital horns of the lateral ventricles, predominantly on the right side and in the third ventricle, leading to the diagnosis of septic shock of probable intracranial origin, and finally to exitus.occipital horns of the lateral ventricles, predominantly on the right side and in the third ventricle, leading to the diagnosis of septic shock of probable intracranial origin, and finally to exitus.
Discussion
We present a case of rhomboencephalitis associated with LM abscess in a healthy subject. This infection should be considered as a diagnostic possibility in elderly patients with immunosuppression. The interest of the case lies in the form of presentation and in the fulminant evolution and course in a patient without immunosuppression, highlighting the parenchymal involvement in the form of abscess and resistance to antibiotic treatment. This is an exceptional case, as only 87 cases of brain abscess due to LM have been described in the literature from 1968 to 2021. Therefore, the diagnosis of LM rhomboencephalitis should be suspected not only in immunocompromised patients, but also in any patient with infectious symptoms and evidence of meningeal or brainstem involvement. The choice of antibiotic treatment is controversial, but a combination of ampicillin and gentamicin for 4 weeks is suggested, and corticosteroids have not been shown to be effective in cases of encephalitis. The presence of abscesses, especially those larger than 2.5 cm, makes it necessary to use surgical drainage and prolong antibiotic treatment for up to 6 weeks.
Conclusion
In Europe, mortality from neurolisteriosis is increasing, explained by the ageing of the population and the increase in the number of immunocompromised patients. The diagnosis of Listeria monocytogenes rhomboencephalitis should be suspected not only in immunocompromised patients, but also in any patient with an infectious condition with evidence of meningeal or brainstem involvement.
It has been found that 20% of affected patients had no risk factors and that in 80% of cases blood cultures were positive, so bacteraemia is almost always found concomitantly, playing an important role in the microbiological diagnostic process of the disease and improving the diagnostic yield together with molecular sequencing techniques.
The most common central nervous system manifestation is meningitis, occurring in 20% of neonates and the elderly, while meningoencephalitis, rhomboencephalitis and cerebritis are less frequent. Brain abscesses are extremely rare and constitute approximately 10% of LM CNS infections, a figure probably underestimated due to limitations in microbiological diagnosis. Furthermore, concomitant meningitis with isolation of this microorganism in CSF occurs in 25-40% of brain abscesses.
In our review of the literature, we found that LM brain abscess is not associated with advanced age and is associated with high mortality (27.3%). In addition, brain stem encephalitis occurs in only 17% of patients, but with a mortality of up to 51%, with the majority of patients with this infectious disease having a fulminant course.
Conflicts of interest statement: No conflicts of interest.
References
- EFSA and ECDC (European Food Safety Authority and European Centre for Disease Prevention and Control), 2019. The European Union One Health 2018 Zoonoses Report. EFSA Journal. 2019; 17: 276.
- Rodríguez-González, María-del-Mar, Marauri-Castillo Iñigo, Armentia-Vizuete Ignacio, Marín-Murillo Flora. “Comunicación de crisis y seguridad alimentaria. Caso listeriosis en la carne mechada”. Rev Profesional de la información 2020; 29: e290605.
- Chung J, McCarthy KL, Redmond A, Butler J, Scott AP, et al. Listeria monocytogenes brain abscess as a late complication of allogeneic haemopoietic stem cell transplantation. Intern Med J.2021; 51: 1005-1006.
- Clauss HE, Lorber B. Central nervous system infection with Listeria monocytogenes. Curr Infect Dis Rep. 2008; 10: 300-6.
- Mylonakis E, Hohmann EL, Calderwood SB. Central nervous system infection with Listeria monocytogenes. 33 years’ experience at a general hospital and review of 776 episodes from the literature. Medicine (Baltimore). 1998; 77: 313-36.