
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
The original nerve of a greater occipital nerve schwannoma causing occipital neuralgia identified with magnetic resonance neurography
Koshi Nakagawa1; Shota Nakashima1; Kentaro Mineji1; Kenji Ishii1; Masanori Ito1; Hironao Yasuoka2; Mitsunori Ozaki1*
11Department of Neurosurgery, Minami Wakayama Medical Center 27-1, Takinai-Machi, Tanabe-Shi, Wakayama 646-8558, Japan.
22Department of Diagnostic Pathology, Osaka Police Hospital 10-31, Kitayama-cho, Tennoji-Ku, Osaka-shi, Osaka 543-0035, Japan.
*Corresponding Author : Mitsunori Ozaki
Department of Neurosurgery, Minami Wakayama Medical Center 27-1, Takinai-machi, Tanabe-shi, Wakayama, ZIP 646-8558, Japan.
Tel: +81-739-26-7050;
Email: ozakim@wakayama-med.ac.jp
Received : Sep 22, 2023
Accepted : Oct 12, 2023
Published : Oct 19, 2023
Archived : www.jcimcr.org
Copyright : © Ozaki M (2023).
Abstract
Schwannomas are benign tumors arising from Schwann cells in the peripheral nerve and rarely develop at suboccipital area. We report a case of a greater occipital nerve schwannoma causing occipital neuralgia. The original nerve of the schwannoma was identified with Magnetic Resonance (MR) neurography. A sixty-something male patient was admitted for a suboccipital mass. Physical examination revealed an about 4 cm beaded masses subcutaneously at suboccipital area. MR imaging showed that the lesions were not suppressed on 3 dimensional T2 weighting with fat suppression. Three dimensional fusion images (3 dimensional T2 weighting with fat suppression and 3-dimensional computed tomography) clearly revealed the original nerve of the lesions. The patient underwent a complete excision on the tumor. Histopathological examination diagnosed it as a schwannoma. The MR neurography findings contributed to preoperatively diagnose the tumors as a greater occipital nerve schwannoma.
Keywords: Peripheral nerve; Benign tumor; Magnetic resonance imaging; Fat suppression.
Citation: Nakagawa K, Nakashima S, Mineji K, Ishii K, Ito M, et al. The original nerve of a greater occipital nerve schwannoma causing occipital neuralgia identified with magnetic resonance neurography. J Clin Images Med Case Rep. 2023; 4(10): 2649.
Introduction
Schwannomas are benign tumors arising from Schwann cells in the peripheral nerve. They usually develop at the head and neck region but rarely at suboccipital area. Moreover it is difficult with imaging examinations to identify the original nerve of a schwannoma at the head and neck region [1,2]. The present case showed the suboccipital mass causing occipital neuralgia. Magnetic Resonance Imaging (MRI) examination demonstrated the tumor originated from the greater occipital nerve. This is the first case whose the original nerve of a greater occipital nerve schwannoma was identified with Magnetic Resonance (MR) neurography.
Case report
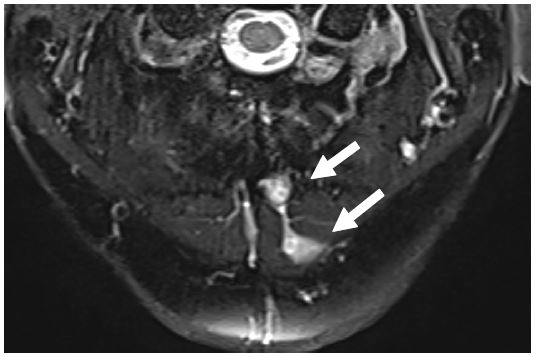
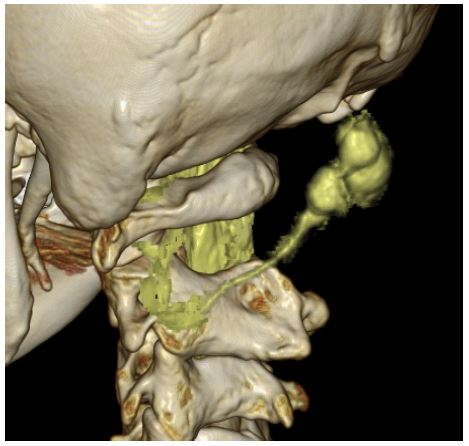
A sixty-something male patient was observed a swelling mass with tenderness with radiation to the top of head in the left upper medial neck, which had been growing for 5 years. Physical examination revealed an about 4 cm beaded masses subcutaneously at suboccipital area. It was firm and immobile. There were no abnormal findings at the skin surrounding the lesions. Ultrasonography showed homogeneous low echoic beaded mass. MRI studying revealed low signal on T1 weighting and enhanced lesion on gadolinium-enhanced imagings. The lesions were not suppressed on 3 dimensional T2 weighting with fat suppression (Figure 1). Three dimensional fusion images (3 dimensional T2 weighting with fat suppression and 3-dimensional computed tomography) at the workstation (Ziostation 2, Ziosoft Inc., Tokyo, Japan) clearly revealed the original nerve of the lesions (Figure 2).
The patient underwent a complete excision on the tumor. He was placed in a prone position under general anesthesia. After linear skin incision, surgical exploration showed gray-pink encapsulated beaded 3 tumors with elastic consistency, measuring 1 cm × 1 cm respectively. The masses were connected to the proximal and distal nerve fibers. The lesions were dissected from the nerve fibers and totally removed. The postoperative course was uneventful.
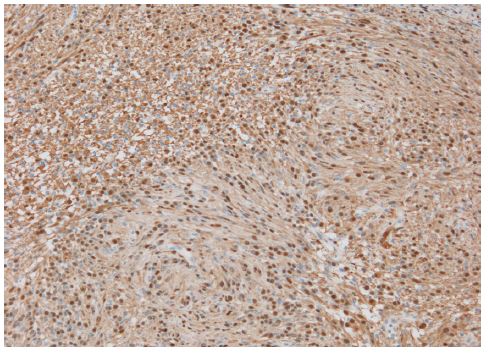
Histopathological report revealed spindle cells with occasional nuclear palisading (Antoni A pattern) and myxomatous cells changes (Antoni B pattern) and positive staining for S-100 protein and it was diagnosed as a schwannoma (Figure 3). No recurrence occurred after 32 months of follow-up. Written informed consent was obtained from the patient for publication of this case report and any accompanying images.
Discussion
The present case is a schwannoma causing occipital neuralgia. The original nerve was identified with preoperative MR neurography. While schwannomas are frequently seen in head and neck region (25-45%), it is rare in suboccipital region [1,2]. As far as we are aware, only 5 cases of greater occipital nerve schwannoma were reported [3-5]. All of them were, however, diagnosed as a greater occipital nerve schwannoma not with the original nerve, but with simply the location. This is the first case whose the original nerve of a greater occipital nerve schwannoma was identified with pre-operative MR neurography.
Occipital neuralgia is a common and sometimes debilitating condition caused by compression, entrapment, or stretching of the occipital nerves. The etiologies of occipital neuralgia were reported such as trauma, cervical spine abnormality and tumor. Osteochondromas, neuromas and multiple myelomas were reported as the cause of occipital neuralgia [6]. Although there are few reports of greater occipital nerve schwannomas, the benign tumors must be kept in mind in the differential diagnosis of patients with occipital neuralgia since they are surgical treatable like the present case.
MR neurography has been shown to have excellent anatomic capability due to the rapid improvements in coil technology and software [7]. With the advancements, it has been possible to follow the peripheral nerve tracts. In the present case, we detect the tumors connected the proximal nerve from C2 cervical nerve posterior fibers. The findings contributed to preoperatively diagnose the tumors as a greater occipital nerve schwannoma. It is extremely useful to diagnose and make a preoperative plan. The further developments of MR neurography are anticipated.
Conclusion
We reported a schwannoma causing occipital neuralgia. The original nerve was identified with preoperative MR neurography. The case is instructive in terms of not only a rare case but also the following of the original nerve of the schwannoma with MR neurography.
References
- M.Apaydin, M Varer, O.T.Kalayci, et al. Large occipital nerve (Arnold’s nerve) schwannoma. JBR-BTR. 2013; 96: 261.
- Beatriz Ballesteros-Del Rio, Adrian Ares-Luque, Javier Tejada-Garcia, et al. Occipital (Arnold) neuralgia secondary to greater occipital nerve schwannoma. Headache. 2003; 43: 804-7.
- Prasad Krishnan, Rajaraman Kartikueyan, Siddhartha Roy Chowdhury, et al. Schwannoma of the greater occipital nerve: An uncommon cause of occipital neuralgia. J Neurosci Rural Pract. 2015; 6: 634-636.
- Si Ying Chrisanda Lee, Ming Yann Lim, et al. Greater occipital nerve schawanoma - A rare cause of occipital neuralgia. Otolaryngology Case Reports. 2020.
- Ural A, Ceylan A, Inal E, Celenk F. A case of greater occipital nerve schwannoma causing neuralgia. Kulak Burun Bogaz Ihtis Derg. 2008; 18: 253-6.
- Cesmebasi A, Muhleman MA, Hulsberg P, et al. Occipital neuralgia: Anatomic considerations. Clin Anat. 2015; 28: 101-8.
- Chhabra A, Zhao L, Carrino JA, et al. MR Neurography: Advances. Radiol Res Pract. 2013; 2013: 809568.