
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Chronic acquired polyneuropathy as presentation of skull based solitary bone plasmacytoma
Naman Agrawal1; Anka Arora1; Sarbesh Tiwari2; Aasma Nalwa3; Sandeep Kumar Bairwa4; Sameer Taywade5; Samhita Panda1*
1Neurology, All India Institute of Medical Sciences, Jodhpur, India.
2Diagnostic and Interventional Radiology, All India Institute of Medical Sciences, Jodhpur, India.
3Pathology, All India Institute of Medical Sciences, Jodhpur, India.
4Medical Oncology, All India Institute of Medical Sciences, Jodhpur, India.
5Nuclear Medicine, All India Institute of Medical Sciences, Jodhpur, India.
*Corresponding Author : Samhita Panda
Additional Professor, Department of Neurology, All India Institute of Medical Sciences, Jodhpur 342005, Rajasthan, India.
Tel: 91-09810838268;
Email: samhitapanda@yahoo.com
Received : Sep 25, 2023
Accepted : Oct 16, 2023
Published : Oct 23, 2023
Archived : www.jcimcr.org
Copyright : © Panda S (2023).
Abstract
Plasmacytomas can be solitary or multiple (osteosclerotic myeloma). Neuropathy resembling chronic inflammatory demyelinating polyradiculoneuropathy or POEMS syndrome has rarely been reported in literature in association of cranial vault plasmacytoma. A female patient with severe demyelinating sensori-motor polyneuropathy with conduction block, was found to have solitary skeletal lesion in the left frontal bone which confirmed to be a plasma cell neoplasm on biopsy. She had significant improvement in neurological signs and symptoms following local radiation and chemotherapy over next 3 months. Solitary bone plasmacytoma (SBP) is rare, accounting for 2-5% of all plasma cell neoplasms. The axial skeleton, especially vertebral body, is the most common site and cranial vault is one of the least commonly reported. Radiation therapy (RT) is the treatment of choice for SBP. There is no evidence that plasma exchange, IVIg or other immunosuppressive agents are effective when used alone in treatment of SBP-associated neuropathy.
What is known?: CIDP associated with plasmacytoma and multiple myeloma is a well described entity. Plasmacytomas are monoclonal gammopathies. They include solitary plasmacytoma of bone, extramedullary plasmacytoma and multiple solitary plasmacytomas. Polyneuropathy may resemble CIDP or be component of POEMS syndrome.
What is new?: The association of cranial vault plasmacytoma with either peripheral neuropathy or POEMS syndrome is very rare. The cranial vault is a rarely described location for SBP. The association of SBP with CIDP like neuropathy without any other clinical clue is very uncommon.
Citation: Agrawal N, Arora A, Tiwari S, Nalwa A, Bairwa SK, Taywade S, Panda S. Chronic acquired polyneuropathy as presentation of skull based solitary bone plasmacytoma. J Clin Images Med Case Rep. 2023; 4(10): 2654.
Introduction
Plasmacytomas are monoclonal gammopathies and include solitary bone plasmacytoma (SBP), extramedullary plasmacytoma and multiple solitary plasmacytomas [1]. SBP affects less than 5% of patients with plasma cell myeloma [2]. We describe a rare presentation of cranial vault plasmacytoma with focus on treatment algorithm and review of literature.
Case report
A right-handed homemaker in her 50s with poorly controlled diabetes mellitus of 2 years, presented with numbness in both lower limbs for 6 months, followed a month later by progressive weakness and pin-pricking sensation in both lower limbs. After 3 months, she complained of numbness in both hands followed by progressive distal weakness in upper limbs, without neck pain, back pain, radicular pain or bladder bowel impairment. There was no fever, weight loss, joint pains, or bony pains, swelling in any part of the body, breast lump or post menopausal bleeding. There were no similar complaints in the past or in her family members.
Neurological examination revealed predominantly distal more than proximal, symmetric weakness in both upper and lower limbs. Power in upper limbs proximally was grade 5/5 (on the Medical Research Council scale), 4/5 distally and 4/5 in proximal lower limbs and 0/5 distally with impaired dorsi- and plantar flexion of both ankles. The sensation to all modalities including touch, pain, temperature, proprioception, and joint position sense was diminished equally (especially in lower extremities) in a length dependent glove and stocking pattern along with absent deep tendon reflexes.
Hematological and biochemical investigations including vitamin B12 levels, thyroid function tests, antiphospholipid antibodies, sntinuclear antibody levels, serum electrophoresis, anti-neutrophil cytoplasmic antibodies, angiotensin-converting enzyme levels, ELISA for IgM Borrelia and erythrocyte sedimentation rate were unremarkable. Serology for HIV, HBV and HCV was normal. Endocrine function tests were normal, except raised HbA1C i.e. 7.3%. laboratory studies showed cerebrospinal fluid (CSF) cell count of 8 per ul with an elevated total protein content (192 mg/dL) and glucose (120 mg/dL). Nerve conduction studies (NCS) showed bilateral symmetrical severe demyelinating sensorimotor polyneuropathy with conduction blocks in both upper and lower limbs, consistent with the diagnosis of CIDP fulfilling the electrodiagnostic criteria proposed by European Federation Neurological Society [5]. Abdominal CT-scan did not reveal organomegaly.
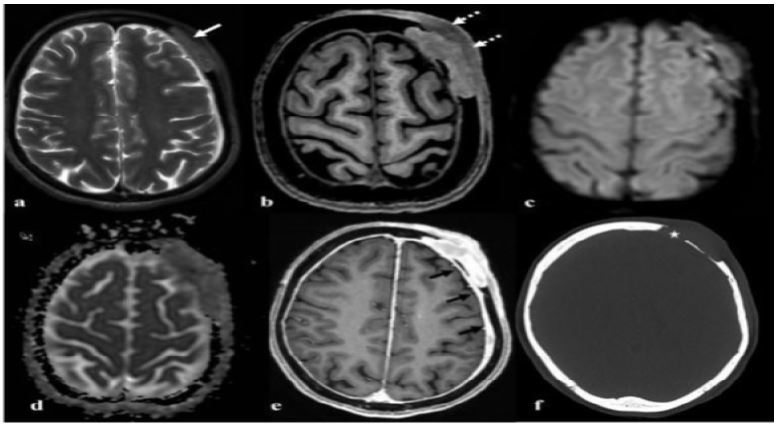
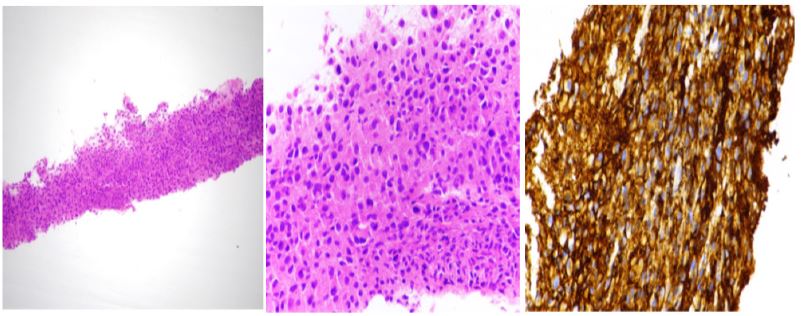
On further evaluation, radiographic skeletal bone survey was done which showed a solitary skeletal lesion in the left frontal bone (Figure 1). Contrast-enhanced MRI brain revealed heterogeneously enhancing mass lesion (Figure 2) involving the frontal bone on left side, possibly plasmacytoma. MRI spine showed mild enhancement of cauda equina nerve roots. 18FDG-PET scan also revealed a metabolically active solitary skeletal lesion in the left frontal bone likely plasmacytoma. Ultrasound guided biopsy of the lesion was done. Histopathology showed cells with eccentrically placed hyperchromatic to coarse round nuclei and moderate to abundant distinct eosinophilic cytoplasm. No necrosis was seen on the sections examined. The tumour cells exhibited strong and diffuse membranous immunopositivity with CD138 suggestive of a plasma cell neoplasm (Figure 3).
Table 1: Literature review for cases of neuropathy associated with SBP of the cranial vault.
| Case | Source | Age | Sex | Duration | Clinical presentation | Provisional diagnosis | Site | CSF protein | Treatment | Outcome |
|---|---|---|---|---|---|---|---|---|---|---|
| 1. | Gherardi et al (1989) [9] | 30 y | F | 2 months | Distal weakness in the lower limbs, particularly in the Plantar flexor of the toes, that is in the distribution of both posterior tibial nerves, the left peroneal nerve appeared to be almost completely spared. There was no sensory deficit. Tendon reflexes were absent in both ankles and the left knee | Mononeuritis multiplex | Single osteolytic, Rounded area located in the parietal region of the skull | 92 mg/dl | Surgical removal and Local radiation (45 Gy). | Symptomatic improvement |
| 2 | Koo et al (2009) [10] | 31 y | M | 3 months | Progressive symmetric motor weakness and sensory dysfunction in the proximal and distal lower limbs with hyporeflexia | CIDP | Focal osteolytic lesion in the parietal bone | 223 mg/dl | Details not given | Details not given |
| 3 | Moss et al (2012) [11] | 43 y | M | 2-3 days | Known case of poems syndrome on the basis of demyelinating polyneuropathy, hepatosplenomegaly, hypogonadism, hyperprolactinemia, hypothyroidism, vitamin D deficiency, adrenal insufficiency, IgA lambda monoclonal proteinemia, skin darkening, a sclerotic bone lesion In the spine, and extra vascular volume overload causing ascites and pleural effusion. Presented with sudden onset vision loss since 3 days | Acute optic neuropathy with POEM syndrome | Enlargement, and enhancement of the left optic nerve and an adjacent enhancing lesion in The suprasellar cistern | 131 mg/dl | Steroid therapy followed by chemotherapy consisting of cyclophosphamide, Bortezomib, and dexamethasone was started. | Symptomatic improvement |
| 4 | Bello et al (2013) [12] | 45 y | M | 2 weeks | Progressive weakness in his lower limbs, absence of reflexes and a loss of superficial sensitivity in his left limb, the presence of enlarged lymph nodes in the cervical area, bilateral gynecomastia, and a hyper pigmentation of the skin | POEM syndrome | Large scalp mass was identified in the parietal-occipital area with intense bone lesion | Not done | Circular craniectomy around the tumour and a complete excision of the lesion by dissecting its adherence with the dura mater, followed by dexamethasone pulse therapy and radiotherapy to the skull | Symptomatic improvement |
| 5 | Sohn et al (2017) [13] | 55 y | F | 6 months | Proximal & distal symmetric, hypotonic areflexic quadriparesis and length dependent sensory loss. | CIDP | Focal osteolytic lesion in the right parietal bone | 219.5 mg/dl | Elective surgical removal of the skull mass | Symptomatic improvement |
| 6 | Gilder et al. (2017) [14] | 47 y | M | 10 years | Hearing Loss, vertigo, and neck stiffness followed by ataxia and length-dependent symmetrical sensory changes in his lower extremities | Cranio-cervical instability | Osteosclerotic lesion centred at the right occipital condyle with extension into the right skull base with involvement of the clivus, occipital bone, and jugular foramen | Not done | Occipital cervical fusion followed by initiation of chemotherapy, he had one cycle of cyclophosphamide and dexamethasone and high dose melphalan and autologous peripheral blood stem cell transplant followed by r definitive surgical fixation | |
| 7 | Present report | 58 y | F | 6 months | Distal symmetric, hypotonic are flexic quadriparesis and length dependent sensory loss | CIDP | Solitary skeletal lesion in left frontal bone | 192 mg/dl | Pulse steroid followed by five cycles of plasmapheresis, after which patient showed mild improvement in neurological symptoms and was planned for local radiation and chemotherapy, after which patient showed significant improvement in neurological signs and symptoms | Symptomatic improvement |

However, the bone marrow biopsy was normal and there was no associated M-band on serum protein and urine electrophoresis. There was no evidence of myeloma related organ or tissue impairment in the form of hypercalcemia, renal insufficiency, anaemia, or compression fractures. The patient was diagnosed as a case of solitary bone plasmacytoma of left frontal bone with acquired demyelinating polyneuropathy.
Suspecting CIDP, the patient was initially started on pulse intravenous steroid therapy followed by five cycles of plasmapheresis but did not show significant improvement in symptoms. Thereafter, on confirmation of the diagnosis, The patient was given local radiation of 45 Gy in 25 cycles and Bortezomib, Lenalidomide and dexamethasone-based chemotherapy.
After completing radiation and chemotherapy she showed significant improvement in neurological signs and symptoms over the next 3 months and markedly improved electrophysiological findings. After 9 months, MRI head showed mild T2/ FLAIR hyperintensity in left frontal bone and did not show any residual lesion. Repeat NCS after 3 months showed improvement in conduction velocities, distal latencies and amplitude and recordable F wave latencies (which were previously non recordable).
Discussion
Polyneuropathy associated with plasmacytoma and multiple myeloma is a well described entity [3,4]. It may resemble chronicinflammatory demyelinating polyradiculoneuropathy (CIDP) [3], or be present as an essential component of the POEMS syndrome (Polyneuropathy, Organomegaly, Endocrinopathy, M-band, Skin changes), a paraneoplastic disorder associated with the presence of a bone plasmacytoma and considered the same entity as osteosclerotic myeloma [4]. The diagnosis of SBP is based on the criteria including absent or minimal M-protein in serum and/or urine, a single area of bone destruction due to clonal plasma cells (on histology), bone marrow not consistent with multiple myeloma, an otherwise normal skeletal survey, MRI of spine and pelvis and no related organ or tissue impairment (including anemia, Hypercalcemia, or renal involvement) [1]. The axial skeleton, especially thoracic vertebral body, is the most common site and the cranial vault as in our case is one of the least commonly reported. While SBP with polyneuropathy is reported, the association of cranial vault plasmacytoma with either peripheral neuropathy or POEMS syndrome has very rarely been reported in literature [6]. There is no evidence that plasma exchange, IVIg or other immunosuppressive agents are effective when used alone in the treatment of SBP-associated neuropathy [7]. However, radiation therapy (RT) remains the treatment of choice for SBP [1]. Our patient was initially treated with standard therapies for immune mediated neuropathy, without much benefit based on the clinical diagnosis. However, with RT after SBP was detected, the patient experienced significant neurological and electrophysiological improvement over 6 months with complete disappearance of lesion 9 months later.
Till date very few cases of neuropathy associated with SBP of cranial vault have been reported, mostly with demyelinating sensori-motor polyneuropathy (Table 1). Almost all of patients had symptoms of neuropathy preceding detection of plasmacytoma and had improvement only after removal of the plasmacytoma while there was little to no benefit with other treatment modalities, skin to our observations. In some cases, it was reported that the patient progressed to develop multiple myeloma on follow up. Even after initial remission of symptoms, the patient needs to be monitored for disease progression both by periodic laboratory and radiological investigations and serum protein electrophoresis as the persistence of M-protein following tumoricidal radiation to an apparent solitary plasmacytoma is reported to confer an increased risk of progression [8]. Multiple myeloma is known to occur in almost 50% of patients with solitary plasmacytoma of bone, most often in the first 3-4 years. However, progression may sometimes be delayed for as long as 15 years [1].
This case highlights that a thorough evaluation is indicated for underlying plasma cell neoplasm in treatment refractory acquired demyelinating neuropathy. The cranial vault is a rare location for SBP and its association with demyelinating neuropathy is uncommon. Therefore, a skeletal survey should be part of the diagnostic evaluation in such patients. Removal of tumour either surgically or through chemo-radiation is associated with symptomatic improvement as immunomodulatory treatment is of limited value. Close observation is recommended for evolution into POEMS syndrome or multiple myeloma even after the removal of the plasmacytoma.
References
- International Myeloma Working Group. Criteria for the classification of monoclonal gammopathies, multiple myeloma and related disorders: A report of the International Myeloma Working Group. British journal of haematology. 2003; 121(5): 749-57. Doi.org/10.1046/j.1365-2141.2003.04355. X.
- Dimopoulos MA, Moulopoulos LA, Maniatis A, Et al. Solitary plasmacytoma of bone and asymptomatic multiple myeloma. Blood, The Journal of the American Society of Hematology. 2000; 96(6): 2037-44. DOI:10.1182/blood.V96.6.2037
- Read DA, Warlow CH. Peripheral neuropathy and solitary plasmacytoma. Journal of Neurology, Neurosurgery & Psychiatry. 1978; 41(2): 177-84. DOI:10.1136/jnnp.41.2.177
- Miralles GD, O’Fallon JR, Talley NJ. Plasma-cell dyscrasia with polyneuropathy: the spectrum of POEMS syndrome. New England Journal of Medicine. 1992; 327(27):1919-23. DOI: 10.1056/NEJM199212313272705.
- Van den Bergh PY, Hadden RD, Bouche P, et al. European Federation of Neurological Societies/Peripheral Nerve Society guideline on management of chronic inflammatory demyelinating polyradiculoneuropathy: Report of a joint task force of the European Federation of Neurological Societies and the Peripheral Nerve Society-first revision. European journal of neurology. 2010; 17(3): 356-63. DOI:10.1111/j.1468-1331.2009.02930.X.
- Scheinker I. Myelom und Nervensystem: Uber eine bisher nicht beschriebene mit eigentümlichen Hautveränderungen einhergehende Polyneuritis bei einem plasmazellulären myelom des Sternums. Deutsche Zeitschrift für Nervenheilkunde. 1938; 147: 247-73. DOI:10.1007/BF01762445.
- Koo YS, Kim BJ. A patient with chronic inflammatory demyelinating polyneuropathy associated with an intracranial plasmacytoma. American journal of physical medicine & rehabilitation. 2010; 89(2): 173-4. DOI: 10.1097/PHM.0b013e3181b33043.
- Wilder RB, Ha CS, Cox JD, et al. Persistence of myeloma protein for more than one year after radiotherapy is an adverse prognostic factor in solitary plasmacytoma of bone. Cancer. 2002; 94(5): 1532-7. DOI:10.1002/cncr.10366.
- Koo YS, Kim BJ. A patient with chronic inflammatory demyelinating polyneuropathy associated with an intracranial plasmacytoma. American journal of physical medicine & rehabilitation. 2010; 89(2): 173-4. DOI: 10.1097/PHM.0b013e3181b33043.
- Gherardi RK, Martin‐Mondiere C, Amiel H, Viard JP, Salama J, Delaporte P. Solitary plasmacytoma of the skull revealed by a mononeuritis multiplex associated with immune complex vasculitis. Arthritis & Rheumatism: Official Journal of the American College of Rheumatology. 1989; 32(11): 1470-3. DOI:10.1002/anr.1780321118.
- Koo YS, Kim BJ. A patient with chronic inflammatory demyelinating polyneuropathy associated with an intracranial plasmacytoma. American journal of physical medicine & rehabilitation. 2010; 89(2): 173-4. DOI: 10.1097/PHM.0b013e3181b33043.
- Moss HE, Liu GT. Acute optic neuropathy associated with an intracranial mass in a patient with POEMS syndrome. Journal of neuro-ophthalmology: the official journal of the North American Neuro-Ophthalmology Society. 2012; 32(1): 45. DOI:10.1097%2FWNO.0b013e318234db5d.
- Plata Bello J, Garcia-Marin V. POEMS syndrome (polyneuropathy, organomegaly, endocrinopathy, multiple myeloma and skin changes) With cranial vault plasmocytoma and the role of surgery in its management: A case report. Journal of Medical Case Reports. 2013; 7(1): 1-5. DOI:10.1186/1752-1947-7-245.
- Sohn SY, Kim JO, Lee SJ. Remission of Chronic Acquired Demyelinating Polyneuropathy Associated With Paraproteinemia After Removal of Skull Plasmacytoma. Journal of Neurology Research.
- Gilder H, Murphy ME, Alvi MA, et al. Skull base plasmacytoma: A unique case of POEMS syndrome with a plasmacytoma causing craniocervical instability. Journal of Clinical Neuroscience. 2018; 47: 254-7. DOI:10.1016/j.jocn. 2017.10.038.