
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Medication conciliation to prevent epilepsy crisis and adverse drug reactions during pregnancy: An emergency case report
Daniele Hermes; Samantha Aline Rauber Bubiak; Cezar Rangel Pestana*
Federal University for Latin-America Integration, Foz do Lguassu, PR, Brazil.
*Corresponding Author : Cezar Rangel Pestana
Federal University for Latin-America Integration, Foz do Iguassu, PR, Brazil.
Email: cezar.pestana@unila.edu.br
Received : Sep 22, 2023
Accepted : Oct 18, 2023
Published : Oct 25, 2023
Archived : www.jcimcr.org
Copyright : © Rangel Pestana C (2023).
Abstract
Background: Medication reconciliation is a pharmaceutical care practice to prevent drug-related problems during pharmacotherapy.
Case: A 16-year-old woman with a 4-year history of epilepsy was admitted to the emergency care unit following two recent seizures episodes with acute headache. The patient was treated with lamotrigine 25 mg plus carbamazepine 200 mg twice daily but is now breastfeeding at 22 days postpartum. A single dose of diazepam 10 mg plus phenobarbital 100 mg once daily were added in order to control seizures. The changes in the response to treatment may reflect changes in pharmacokinetics or presence of drug interaction during pregnancy. It is also well known that phenobarbital can induce drug metabolism and accelerate drug elimination.
Conclusion: In such cases, medication reconciliation is essential in order to optimise response to medication and to prevent drug-related problems.
Keywords: Drug interaction; Medication reconciliation; Pharmaceutical care; Women´s health.
Teaching Points: Medication conciliation reduces drug interaction; Relevance of pharmaceutical care during pregnancy; Promotion of pregnancy healthcare.
Citation: Hermes D, Rauber Bubiak SA, Rangel Pestana C. Medication conciliation to prevent epilepsy crisis and adverse drug reactions during pregnancy: An emergency case report J Clin Images Med Case Rep. 2023; 4(10): 2658.
Introduction
Epilepsy is a brain disorder that predisposes patient to seizures episodes. The diagnosis is based on clinical symptoms, electroencephalogram and other imaging exams [1-3]. Carbamazepine (CBZ) and Lamotrignine (LTG) are highly effective antiepileptic drugs used to treat seizure disorders. Its pharmacological activity involves the blockage of sodium-dependent depolarization and inhibition of spinal cord and cortex [4,5].
Studies have demonstrated that changes in the LTG pharmacokinetics during pregnancy of epileptic patients [6,7]. Plasma concentration of Lamotrigine is particularly affected by changes in clearance during pregnancy [8,9]. Medication reconciliation is a pharmaceutical care practice consisted of collecting information about current medication used by patients to compare with new prescriptions in order to prevent drug-related problems during pharmacotherapy [10].
Case presentation
A 16-years-old postpartum woman was admitted at an emergency care unit after two seizures episodes even upon continued treatment with CBZ 200 mg and LTG 25 mg twice a day. The patient received intravenously 2 ml of dipyrone (metamizole) 500 mg/mL plus 2 ml of sodium hydrochloride metoclopramide 5 mg/mL. After 12 hours observation, she was discharged but seizures episodes continued in the next day.
A new prescription containing a single oral dose of Diazepam 10 mg plus Phenobarbital (PHE) 100 mg once a day was included in her pharmacotherapy as illustrared in Figure 1. Supplementary skull computed tomography exam and blood biomarkers analysis were recommended to exclude other brain injuries or abnormalities related to the symptoms.
The persistent seizures episodes suggest potential changes in therapy response to LTG and CBZ during pregnancy or postpartum. In order to control convulsive crisis PHE was additionally prescribed despite barbiturates has the ability to cause clinically relevant drug interactions to antiepileptic drugs [11]. As sleepiness is a side effect among individuals taking phenobarbital, the patient was oriented to sleep at least four streak hours a day and avoid bathing or ridding the baby unaccompanied.
Alanine Aminotransferase (ALT) and Aspartate Aminotransferase (AST) plasmatic determination are widely used biomarkers to assess potential hepatic dysfunction during anticonvulsivant treatment. Despite ALT and AST are not associated with changes in CYP biotransformation capacity, its determination evaluates potential liver toxicity caused by antiepileptic drugs [12]. Table 1 shows serum biomarkers determination did not reveal any significant changes in hemogram as well as liver and kidney function, except for the presence of glucose in urine (Table 1).
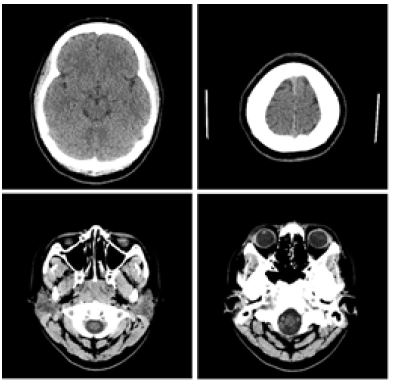
Computed Tomography (CT) is commonly used as a supplementary imaging exam to investigate seizure caused by intracerebral hemorrhage. Patients diagnosed with epilepsy are generally assessed by Magnetic Resonance Imaging which identifies epileptogenic lesions with structural abnormalities [13]. Figure 2 shows CT images from telencephalic parenchyma with normal attenuation coefficients, preserved cortical sulci, fissures and basal cisterns. Also, ventricular system morphology and dimensions were ascribed as normal. Intra or extra axial expansive lesions were not found as well as any abnormal parenchymal calcification (Figure 2).
Despite mothers with epilepsy are more likely to not breastfeeding, antiepileptic drugs are not contraindicated, so it was emphasized the importance of maternal milk to children development [14]. The treatment of persistent epilepsy crises requires a better investigation regarding to factors potentially related to changes in antiepileptic plasma levels. Adherence to the treatment must also be clearly confirmed once administration errors are one of the main cause of treatment failure. It is also important to emphasize that special group patients such as pregnant should be periodically examined regardless the existence of seizures crises in order to achieve more effective and safe treatment.

Table 1: Determination of clinical blood biomarkers to investigate changes in liver and kidney functions.
| Determination | Quantification | Reference |
|---|---|---|
| Eritrocytes | 4.11 mm3 | 4.10 to 5.10 |
| Leucocytes | 10.45 mm3 | 5.0 to 10.0 mm3 |
| Platelets | 356.0 mm3 | 140 to 400 mm3 |
| Urine | Glicose + | not detected |
| Urea | 21 mg/dL | 15 to 36mg/dL |
| Creatinine | 0.70 mg/dL | 0.52 to 1.04 mg/dL |
| Sodium | 140 mmol/L | 136 to 145 mmol/L |
| Potassium | 4.1 mmol/L | - |
| AST | 19 U/L | 5 to 30 U/L |
| ALT | 10 U/L | < 35 U/L |
| PT | 25.2 sec | 25 to 32.3 sec |
| APT | 100%, INR=1 | 70 to 100 %, INR<1.5 |
| CRP | 0.5 mg/dL | < 1.0 mg/dL |
AST: Aspartate Aminotransferase; ALT Alanine Aminotransferase; PT: Prothrombin Time; APT: Actived Prothrombin Time; CRP: C-Reactive Protein.
Discussion
The present case report shows a puerperal patient with persistent seizure episodes likely caused by changes in therapy response to entiepleptic drugs. In addition, the use of phenobarbital brought additional risk of drug interactions with relevant clinical outcomes. These findings demonstrate maternal pharmaceutical care are fundamental to prevent adverse drug reactions in pregnancy therapy.
Declarations
Acknowledgements: We thank Pro-Reitoria de Pesquisa e Pós-Graduação from Universidade Federal da Integração Latino Americana for the financial support.
Conflict of interest: No conflict of interest to declare.
Consent to publish: All authors have agreed with manuscript submission and patient consented to publication.
References
- Krumholz A, Wiebe S, Gronseth GS, et al. Evidence-based guideline: management of an unprovoked first seizure in adults: report of the guideline development subcommittee of the American Academy of Neurology and the American Epilepsy Society. Epilepsy Curr. 2015; 15: 144-152.
- Magnusson C, Herlitz J, Hoglind R, et al. Prehospital lactate levels in blood as a seizure biomarker: a multi-center observational study. Epilepsia. 2021; 62: 408-415.
- Matz O, Heckelmann J, Zechbauer S, et al. Early postictal serum lactate concentrations are superior to serum creatine kinase concentrations in distinguishing generalized tonic-clonic seizures from syncopes. Intern Emerg Med. 2018; 13: 749-755.
- MacDonald RL, Kelly KM. Antiepileptic drug mechanisms of action. Epilepsia. 1995; 36: S2-S12.
- Kuo CC, Chen RS, Lu L, Chen RC. Carbamazepineinhibition of neuronal Na+currents-quantitative distinction from phenytoin and possible therapeutic implications. Mol Pharmacol. 1997; 51: 1077-1083.
- Öhman I, Beck O, Vitols S, Tomson T. Plasma concentrations of lamotrigine and its 2-N-glucuronide metabolite during pregnancy in women with epilepsy. Epilepsia. 2008; 49: 1075-1080.
- Petrenaite V, Sabers A, Hansen-Schwartz J, Individual changes in lamotrigine plasma concentrations during pregnancy, Epilepsy Res. 2005; 65: 185-188.
- Richards N, Reith D, Stitely M, Smith A. Are doses of lamotrigine or levetiracetam adjusted during pregnancy? Epilepsia Open. 2017; 3: 86-90.
- Wang M, Tao Y, Sun X et al. Estrogen profile- and pharmacogenetics-based lamotrigine dosing regimen optimization: Recommendations for pregnant women with epilepsy, Pharmacol Res. 2021; 169.
- Magalhães GF, De Santos GBNC, Rosa MRB, et al. Medication reconciliation in patients hospitalized in a cardiology unit. PloS One. 2014; 9: 1-12.
- Armijo JA, Bravo J, Cuadrado A, Herranz JL, et al. Lamotrigine serum concentration-to-dose ratio: Influence of age and concomitant antiepileptic drugs and dosage implications. Ther Drug Monit. 1999; 21: 182-90.
- Vidaurre J, Gedela S, Yarosz S. Antiepileptic drugs and liver disease. Pediatr Neurol. 2017; 77: 23-36.
- Salmenpera TM, Duncan JS. Imaging in epilepsy. J Neurol Neurosurg Psychiatry. 2005; 76: iii2-iii10.
- Belfort MB, Knight E, Chandarana S, et al. Associations of Maternal Milk Feeding With Neurodevelopmental Outcomes at 7 Years of Age in Former Preterm Infants. JAMA Netw Open. 2022; 5: e2221608.