
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Known case of ESRD due to IgA nephropathy with myelodysplastic syndrome having perinephric hematoma and disseminated multi-drug resistant Klebsiella pneumonia infection in urinary tract, gastrointestinal tract and testes following living donor kidney transplantation: The strength of multidisciplinary team management
Khin Phyu Pyar1; Aung Kyaw Tun2; Chann Myei3; Kyaw Thura4; Aung Htet5; Aung Zaw Htet6; Aung Aung7;
Zar NiHtet Aung8; Aung Thu8; Kyaw Thet Maung8; Kyaw Thu Yein Lwin6; Lay Maung Maung6;
Thein Tun Myint8;Tun Tun Oo9; Myat Ko Ko9;
Sitt Min8; Zaw Min Htike10
1Professor and Head/Senior Consultant Physician and Nephrologist, Department of Medicine/Nephrology, Defence Services Medical Academy/ No. (1) Defence Services General Hospital (1000-Bedded), Yangon, Myanmar.
2Consultant Uro-surgeon, Department of Urology, No. (1) Defence Services General Hospital, Yangon, Myanmar.
3Consultant Intensivist, Department of Anaesthesia, No. (1) Defence Services General Hospital, Yangon, Myanmar.
4Consultant Cardiovascular-surgeon, Department of Cardiac surgery, No. (1) Defence Services General Hospital, Yangon, Myanmar.
5Consultant Radiologist, Department of Radiologist, No. (1) Defence Services General Hospital, Yangon, Myanmar.
6Consultant Nephrologist, Department of Nephrology, No. (1) Defence Services General Hospital, Yangon, Myanmar.
7Consultant Hematologist, Department of Hematology, No. (1) Defence Services General Hospital, Yangon, Myanmar.
8Consultant Physician, Department of General Medicine, No. (1) Defence Services General Hospital, Yangon, Myanmar.
9Nephrology Fellow, Department of Nephrology, Defence Services Medical Academy, Yangon, Myanmar.
10Consultant Microbiologist, Department of Microbiology, No. (1) Defence Services General Hospital, Yangon, Myanmar.
*Corresponding Author : Khin Phyu Pyar
Professor and Head/ Senior Consultant Physician and Nephrologist, Department of Medicine/Nephrology, Defence Services Medical Academy/ No. (1) Defence Services General Hospital (1000-Bedded), Yangon, Myanmar.
Email: khinphyupyar@gmail.com
Received : Sep 29, 2023
Accepted : Oct 23, 2023
Published : Oct 30, 2023
Archived : www.jcimcr.org
Copyright : © Pyar KP (2023).
Abstract
A 34 years old man, had increasing pain over grafted kidney with low urine output on post-operative ‘Day 7’ following living donor kidney transplantation. He was a known case of IgA nephropathy with end stage renal disease and Myelodysplastic Syndrome (MDS). CT abdomen revealed perinephric hematoma; cast effect on graft kidney; and the density over grafted kidney was decreased suggestive of rejection. He also had disseminated multi-drug resistant Klebsiella pneumonia infections in urinary tract, gastrointestinal tract and orchitis. Multi-disciplinary team’s management which includes nephrologists, general physicians, hematologists, uro-surgeons, vascular surgeons, radiologists, microbiologists and anesthetists saves patient’s life as well as transplant kidney.
Keywords: Myelodysplastic syndrome; Perinephric hematoma; Disseminated infections; Multi-drug resistant klebsiellapneumonia; Rejection; Multi-disciplinary team.
Citation: Pyar KP, Tun AK, Myei C, Thura K, Htet A, et al. Known case of ESRD due to IgA nephropathy with myelodysplastic syndrome having perinephric hematoma and disseminated multi-drug resistant Klebsiella pneumonia infection in urinary tract, gastrointestinal tract and testes following living donor kidney transplantation: The strength of multidisciplinary team management. J Clin Images Med Case Rep. 2023; 4(10): 2663.
Introduction
The incidence of chronic kidney disease is expected to be 10% of total population; and the number End Stage Renal Disease (ESRD) is increasing. Kidney transplant is accepted as preferred treatment option among three renal replacement therapies: Hemodialysis, peritoneal dialysis and renal transplant.
Myelodysplastic Syndrome (MDS) is an acquired clonal hematopoietic cell disorder, clinically characterized by ineffective hematopoiesis leading to various degrees of cytopenia, dysplastic morphology in the bone marrow, and a tendency to transform into acute myelogenous leukemia. The prevalence of MDS was increased in patients with ESRD if the duration of hemodialysis was longer and the requirement for blood transfusion was increased [3].
To prevent rejection of grafted kidney, immunosuppressants play a key role. The effect of immunosuppressant therapy on bone marrow is anemia (mycophenolate mofetil), leucopenia (mycophenolate mofetil) and thrombocytopenia (mycophenolate mofetil). Moreover, the induction agents like ATG and Basiliximab have bone marrow suppressant effect through immune mediated mechanism.
Therefore, doing renal transplant in patient with MDS is very challenging. This case report described fatal effect of white cell defect and low platelet count on recipient himself and grafted kidney; disseminated multi-drug resistant Klebsiellapneumonia infections.
Case presentation
At the age of 29 year, the patientcame with high blood pressure and raised serum creatinine (2 mg/dl). IgA nephropathy was diagnosed in renal biopsy done in 2017; mesangial proliferation; focal segmental endocapillary proliferation; IFTA (30%); MEST C score M1, E1, S1, T1, C1. He was treated with intravenous methylprednisolone followed by oral prednisolone and monthly cyclophosphamide infusion for 6 months. Renal biopsy was repeated in 2018 as proteinuria was persistent; it revealed mesangio-proliferative glomerulitis; and IFTA (30%). He did not attend follow up for 2 years.
Three years later, in November 2020, he presented with sky high blood pressure together with uremic symptoms; serum creatinine was 9 mg/dl. Therefore, hemodialysis was initiated. His blood pressure ranged from 260/140 to 160/100 mmHg; it required 8 antihypertensives including 2 diuretics. He had target organ involvements in heart and retina; Grade II hypertensive retinopathy; and left ventricular hypertrophy. In 2022, he was investigated for prolonged fever and refractory anemia; Myelodysplastic Syndrome (MDS) was diagnosed after doing bone marrow examination. He received 2 units of blood transfusion prior to transplant.
The residual urine output was almost nil for 4 months. He required 8 drugs to control blood pressure. He was on Telmisarten 80 mg OD, PO Nifedipine 60 mg BD, PO Duracard 4 mg QID, PO Aldomet 500 mg QID, PO Aldactone 25 mg BD, PO Cardivas 25 mg BD, PO Hydralazine 50 mg QID, PO Lasix 125 mg BD, PO Aspilet 1 OD, PO Atorvas 10 mg HS, PO Seva 800 mg BD.
As the test for tuberculosis (IGRA) was positive, he was prescribed with antitubercular therapy for 3 months prior to transplant. His chest radiograph did not reveal parenchymal lesion. His BMI was 17.9 kg/m2; his dry weight was 50.2 kg and height was 5 ft 6 inches. ECG was normal. Mild cardiomegaly was noted in chest radiograph. Echocardiogram showed moderate concentric LVH with Grade I diastolic dysfunction; good LVEF (67%); and, there was no wall motion abnormality. His hemoglobin was 10.9 gm%; total WBC was 4.6x109/L; platelet count was 124x109/L. Carotid doppler revealed calcified atheromatous plaque in left carotid bulb. He received blood group matched non-related living donor who was 18 years old. CDC cross match was negative; however, in tissue typing (Luminux), there were unspecified HLA antibody. The highest MFI was 9100; CREG (7) was positive; the lowest MFI was 2295; and there was no Donor Specific Antibody (DSA).
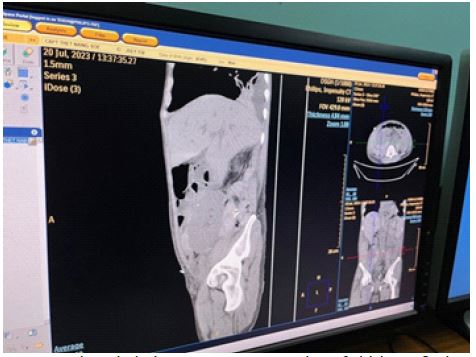
His platelet count prior to transplant was stable at 120x109/L; it dropped to 70x109/L on post-operative ‘Day 3’ and it was corrected with single donor platelet transfusion. The patient’s wife noticed a large area of ecchymosis on immediate post-operative period. (Figure 1) Patient noticed lower abdominal discomfort on ‘Day 7’; it gradually increased in severity and right upper thigh was swollen by ‘Day 10’. USG was compatible with cellulitis with normal RI on ‘Day 7’; it showed increasing soft tissue swelling on ‘Day 10’. As he had pain over transplant area, CT abdomen was done. It revealed perinephric hematoma at graft kidney; and impending ‘cast effect’ on graft kidney from surrounding hematoma (Figures 3-7). Moreover, the density over grafted kidney was decreased suggestive of rejection.Therefore, it indicated acute rejection too.
In view of possible pressure effect on grafted kidney (compression of the renal collecting system, of the vascular pedicle, or to graft dysfunction) which would reduce blood supply, discussion among transplant team members was done. Uro-surgeon would like to open again and remove the clots in order to reduce pressure effects; however, the chances of re-accumulation was unavoidable. The anesthetist mentioned the risks of repeating another surgery; and possible chance of acquiring infection. The vascular surgeon explained that the cause of hematoma was unlikely to be bleeding from artery or venous origin in view of its gradual onset. The hematologist agreed to correct platelet count as the most likely cause for hematoma was thrombocytopenia; it dropped from pretransplant count of 120x109/L to 70x109/Lon post-transplant ‘Day 7’. The radiologist suggested torepeat CT abdomen after correction of platelet count. Nephrologists and general physicians agreed to continue conservative treatment on perinephric hematoma and close monitoring of urine out-put, the amount of drain from drainage tube, serum creatinine and hematological parameters in addition to local abdominal signs clinically.
Therefore, low platelet count was corrected with one unit of single donor platelet and packed cell accordingly. Other bleeding profiles (BT, CT, PT, INR, APTT) were done too. Parenteral steroid therapy was extended for another 3 days.
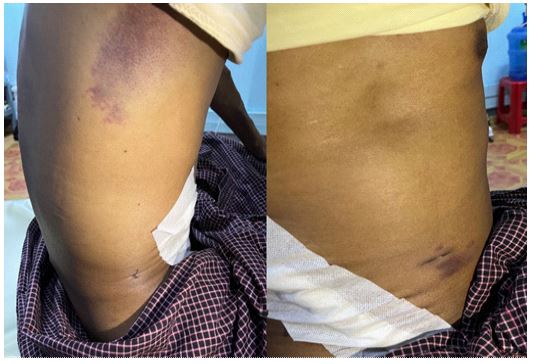





Moreover, on Day ‘10’, he had one spike fever; his right scrotum became swollen and tender (Figure 2). Antimicrobial therapy was indicated as he had one spike of fever with rise in total WBC count. The culture results from urine, done after removal of catheter (Day 7), revealed ESBL; all beta lectin resistant except cephamycin; phenotype Klebsiella pneumonia; it was sensitive to aminoglycoside, fosfomycin and imipenem. He had loose motion. Stool examination showed bacteria without trophozoite or cyst. Moreover, stool culture showed Carbepenem resistant Klebsiellapneumonia; it was sensitive to amikacin. Therefore, he had disseminated multi-drug resistant Klebsiellapneumonia infection in urine, right testes and stool. Colistin had intermediate sensitivity in both culture; therefore, he was given in colistin for two weeks. Close monitoring was done.
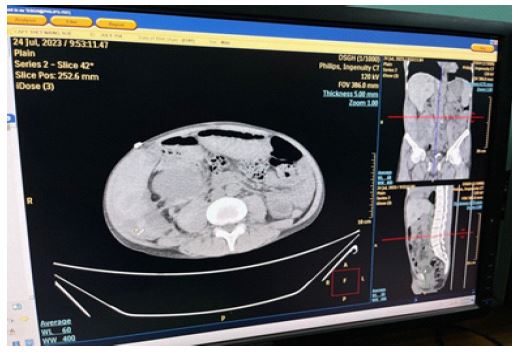
Third day after correction of platelets, local abdominal distension decreased; the drain color was clear; the urine volume increased; serum creatinine dropped; platelet count rose to 100x109/L; hemoglobin was stable at 11 gm%; CT scan finding improved. Recheck CT scan revealed no extension of hematoma; the density of hematoma was compatible with more of old blood; the density of grafted kidney was improving (Figures 8 and 9). The patient went home on ‘Day 30’ after transplant; serum creatinine was 1.14 mg%; hemoglobin was 12.3 gm%; platelet count was 302X109/L; daily urine output was 5,000 cc.

Discussion
The study on MDS done in Taiwan found that undergoing dialysis and age had positive predictive value for MDS occurrence. Moreover, more units of red blood cell transfusion (higher than 4 units per month) was also associated with a higher incidence of MDS; the MDS cumulative incidence increased with the duration of dialysis in ESRD patients [3]. However, in this patient, the dialysis vintage was 2 years. In patients with ESRD, the chances of MDS was increased if they required one unit of blood transfusion per week i.e., refractory anemia with adequate erythropoietin therapy and iron replacement [3]. In this patient, he had only 2 units of blood transfusion over 2 years; rare case.
This is one reason for case reporting. This patient underwent surgery after maintaining low normal platelet count for two weeks. However, he had a large ecchymosis over right axillaon immediate post-operative period. Therefore, it must be due to qualitative defect of platelets; the cause of the qualitative defect of platelets may result from MDS as well as ESRD. It showed that both quantity and quality of platelets were important in bleeding. This is another reason for case reporting.
Because of low platelet count and perinephric hematoma, platelet transfusion was done in this patient. Platelet transfusion may result in production of auto-antibody to platelet which might attack grafted kidney. It may cause delay graft function in acute phase as well as chronic rejection. The chances of rejection in this patient being associated with MDS, may be more likely than that of kidney transplant recipient without MDS. Both the transplant physician and the patient himself must have awareness of rejection risks. This is third reason for writing this case.
Currently, ultrasound of grafted kidney is included in protocol because it can shows features of rejections; a graft oedema and increased volume; rounded, hypoechoic pyramids; and sometimes prominent papilla; diminished diastolic flow is detected in the intrarenal arteries due to increased distal resistance secondary to endothelial infiltrate in vascular rejection; interstitial swelling in cellular rejection; and a resistive index higher than 0.80 is suggestive of acute rejection in the appropriate clinical setting [5]. However, having subcutaneous hematoma over grafted kidney had reduced visual field; CT scan abdomen was done. Early detection of renal allograft complications is important for long-term graft survival.
CT abdomen plays an important role in imaging of grafted kidney; it demonstrates perinephric hematoma; pressure effect; whether there is ongoing hemorrhage or not. Apart from the effect of radiation, doing non-contrast CT abdomen is very informative [2,11,12]. We would like to disseminate the role of CT scan in transplant recipient; it gave early diagnosis of hematoma as well as graft kidney; response to treatment; the importance of imaging in renal transplant. It highlighted that radiology plays an essential role in diagnosis as well as response to treatment in renal transplant.
Furthermore, it can also show diffuse parenchymal complications (acute rejection, acute tubular necrosis and nephrotoxicity) by comparing the density with nearby muscle density. Because of subcutaneous hematoma, doing ultrasound of graft kidney in this case was not informative. Moreover, doing biopsy from graft kidney is included in transplant protocol in immediate transplant period; acute anti-body mediated rejection and cell mediated rejection have different form of treatment and histopathology with special stains are essential. However, doing biopsy is contraindicated in patient with low platelet count- like this case. Therefore, having CT features of rejection with high serum creatinine and low urine output confirmed delayed graft function. We did repeat parenteral steroid for rejection and the patient recovered. This is another reason for sharing usefulness of CT in graft kidney. It gave practical evidence to the suggestions by Ghonge and colleagues that radiologists are integral part of multidisciplinary transplantation team [4].
Timely diagnosis and making decision for the best appropriate treatment with local logistics was extremely important for prevention of acute rejection as well as chronic graft failure when the patient had acute crisis; perinephric hematoma with potential pressure effect on graft kidney; low platelet counts (70x109/L); relatively high total WBC count with neutrophil dominant (11.1x109/L); multi-drug resistant Klebsiellapneumonia septicemia (urine and stool) and septic orchitis; and raised serum creatine. We do appreciate the kindness; readiness; enthusiasm; and collaboration of all transplant team members. This case report highlighted the value of multi-disciplinary team: Nephrologists, general physicians, hematologists, uro-surgeons, vascular surgeons, radiologists, microbiologist, intensivists and anaesthetists.
The patient also had disseminated multi-drug resistant Klebsiellapneumonia infection in urine, testes and stool. Reasons for having disseminated bacterial infection in this patient was multi-factorial in etiology; qualitative dysfunction of WBC; quantitative defect of WBC; immune defect in MDS; immunocompromised state due to triple immunosuppressant therapy (steroids, mycophenolate mofetil and tacrolimus).
This case also highlighted the problem of anti-microbial resistance among notorious bacteria, Klebsiellapneumonia. In the urine culture, phenotype klebsiella pneumonia was detected; it was resistant to all beta lactam except cephamycin; it was sensitive to aminoglycoside, fosfomycin and imipenem. Moreover, stool culture showed carbepenem resistant klebsiella pneumonia; it was sensitive to amikacin. As aminoglycosides are nephrotoxic, it is dangerous to prescribe amikacin to renal transplant recipient with delayed graft function. It was not easy to monitor blood level of amikacin in low resource setting in daily basis. Therefore, we choose colistin as it showed intermediate sensitivity in both urine and stool culture. Right sided orchitis was probably due to Klebsiellapneumonia septicemia with bacteria orchitis. Thus, he had disseminated multi-drug resistant klebsiellapneumonia infection in urine, testes and stool. Features of inflammation in right testes became gradually subsided over 3 days. And, he was given Colistin for two weeks.
Nearly 30% of cases with MDS were found to have chronic kidney disease [8] they might progress to ESRD and required renal replacement therapy. Doing renal transplant in known case of MDS was very challenging. Myelodysplastic Syndrome (MDS) is a heterogeneous hematological disorder characterized by a spectrum of clinical presentation, cytogenetic, and somatic gene mutations and the risk of transformation to acute leukemia. Management options include observation, supportive care, blood transfusion, administration of growth factors and/or hypomethylating agents and Hematopoietic Cell Transplant (HCT) either upfront or after disease progression. This patient was very young, 34 years; the median age of diagnosis of MDS in one study was 70 years [1,7] Two case reports on renal transplant recipients with azathioprine developed MDS 10-16 years after renal transplant [10]. Their suggestion was “if patients with long term azathioprine treatment show progressive pancytopenia, one should suspect the possibility of myelodysplastic syndrome” [6]. In another case report suggested to do both bone marrow transplant and renal transplant in a case of MDS with ESRD; a Human Leukocyte Antigen (HLA)-Haploidentical Allo Hematopoietic Cell Transplantation (alloHCT) and a kidney transplant from same haploidentical sibling donor [9].
Conclusion
Doing renal transplant in patients with MDS is very challenging particularly without prior bone marrow transplant. Imaging plays a key role in routine surveillance and in management of acute or chronic transplant dysfunction. This case report highlighted the value of multi-disciplinary team: Nephrologists, general physicians, hematologists, uro-surgeons, vascular surgeons, radiologists, intensivists and anesthetists. Early diagnosis and treatment of complications in renal transplant recipient are paramount to prevent graft failure and other significant morbidities to the patients.
Declarations
Acknowledgements: The authors would like to thank the patient and family for giving consent to this article. Also, to all doctors and nursing team for making great efforts in caring her. The authors acknowledged the following team; Professor Yu Aye Latt and anesthetic team; Professor Ohmar Hlaing and radiology team; Professor Tin Moe Mya and laboratory team; Professor Myint Zaw, Professor Thet Naing, Professor Kyaw ZayYa and Professor Ko Ko Lwin for administrative support.
Declaration of conflict of interest : The authors declared no potential conflicts of interests with respect to authorship and publication of this article.
Ethical approval: Our institution does not require ethical approval for reporting cases.
Funding: The authors received no financial support for publication of this article.
Informed consent: The informed consent for publication in this article was obtained from both recipient and donor.
References
- Arslan S, Nakamura R. Decision Analysis of Transplantation for Patients with Myelodysplasia: “Who Should We Transplant Today?”. Current Hematologic Malignancy Reports. 2020; 15: 305–315. https://doi.org/10.1007/s11899-020-00573-6
- Benjamens S, Glaudemans AWJM, Berger SP, Slart RHJA, Pol RA. Have we forgotten imaging prior to and after kidney transplantation? European Radiology. 2018; 28: 3263–3267. https://doi.org/10.1007/s00330-018-5358-5356
- Chang MY, Lin SF, Wu SC, Yang WC. Myelodysplastic syndrome: The other cause of anemia in end-stage renal disease patients undergoing dialysis. Scientific Reports. 2020; 10: 15557. https://doi.org/10.1038/s41598-020-72568-72575
- Ghonge NP, Goyal N, Vohra S, Chowdhury V. Renal transplant evaluation: Multimodality imaging of post-transplant complications. The British Journal of Radiology. 2021; 94: 20201253. https://doi.org/10.1259/bjr.20201253
- Inci MF, Ozkan F, See TC, Tatli S. Renal Transplant Complications: Diagnostic and Therapeutic Role of Radiology. Canadian Association of Radiologists Journal. 2014; 65: 242–252. https://doi.org/10.1016/j.carj.2013.06.002
- Kwon HS, Yoon SN, Yang CW, Lee SH, Kim YS, Kim SY, et al. Myelodysplastic Syndrome in a Renal Transplant Recipient Treated with Long-term Azathioprine. Korean Journal of Nephrology. 1997; 16: 412–416.
- Lafargue MC, Van Huyen, JPD, Isnard P, Rennke H, Essig M, Bobot M, et al. #2663 KIDNEY INVOLVEMENT IN MYELODYSPLASTIC SYNDROMES. Nephrology Dialysis Transplantation. 2023; 38: gfad063c_2663. https://doi.org/10.1093/ndt/gfad063c_2663
- Lucijanic M, Krecak I, Kusec R. Renal disease associated with chronic myeloproliferative neoplasms. Expert Review of Hematology. 2022; 15: 93–96. https://doi.org/10.1080/17474086.2022.2039117
- Miller KC, Hall AC, Cohen-Bucay A, Chen YB. Delayed kidney transplantation after HLA-haploidentical hematopoietic cell transplantation in a young woman with myelodysplastic syndrome with renal failure. Leukemia Research Reports. 2022; 17: 100302. https://doi.org/10.1016/j.lrr.2022.100302
- Shiraishi J, Sudo Y, Katori Y, Akiyama M, Takada O, Maki K, et al. Myelodysplastic Syndrome (RAEB in T) Developed in a Renal Allograft Recipient. Rinsho Ketsueki. 1998; 39: 600–605. https://doi.org/10.11406/rinketsu.39.600
- Sjekavica I, Novosel L, Rupčić M, Smiljanić R, Muršić M, Duspara V, et al. RADIOLOGICAL IMAGING IN RENAL TRANSPLANTATION. Acta Clinica Croatica. 2018; 57: 694–712. https://doi.org/10.20471/acc.2018.57.04.12
- Valdair Francisco Muglia, Sara Reis Teixeira, Elen Almeida Romão, Marcelo Ferreira Cassini, Murilo Ferreira de Andrade. Imaging in Kidney Transplantation. In Thomas Rath (Ed.), Current Issues and Future Direction in Kidney Transplantation (p. Ch. 2). Intech Open. 2013; https://doi.org/10.5772/55074.