
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Granulomatous panniculitis in the setting of histoplasmosis in a patient with dermatomyositis on immunosuppressants
Troy Selvaratnam1*; Alejandro Matos Wells2; Timothy Blackwell3; Asena Bahce-Altuntas4; Mariela Mitre3; Bindu Balani2
1St. George’s University School of Medicine, Grenada, West Indies.
2Infectious Diseases, Hackensack School of Medicine, Hackensack University Medical Center, Nutley, NJ, USA.
3Dermatology, Hackensack School of Medicine, Hackensack University Medical Center, Nutley, NJ, USA.
4Rheumatology, Hackensack School of Medicine, Hackensack University Medical Center, Nutley, NJ, USA.
*Corresponding Author : Troy Selvaratnam
St. George’s University School of Medicine, Grenada, West Indies.
Tel: +1-646-206-2355.
Email: tselvara@sgu.edu
Received : Sep 26, 2023
Accepted : Oct 24, 2023
Published : Oct 31, 2023
Archived : www.jcimcr.org
Copyright : © Selvaratnam T (2023).
Abstract
This report describes a case of panniculitis in the setting of infection with histoplasma capsulatum in a patient with active dermatomyositis on immunosuppressive medications. The appearance of panniculitis on the patient’s lower extremity was interpreted as possible necrotizing cellulitis in the setting of the patient’s immunosuppressive therapy or worsening of her dermatomyositis rash. The patient was placed on multiple trials of empiric antibiotic therapy for over a month with no improvement of her plaques. The patient did not exhibit the typical clinical manifestations of histoplasmosis nevertheless, through further workup, including, histological studies and sterile tissue culture, the patient was ultimately found to be infected with H. capsulatum and initiated on antifungal therapy. The case emphasizes the importance of placing other uncommon infectious etiologies like histoplasmosis on the differential in myositis patients on immunosuppression therapy with atypical presentations. Timely consideration of such possibilities ensures that appropriate therapies are initiated without delay.
Citation: Selvaratnam T, Wells AM, Blackwell T, Altuntas AB, Mitre M, et al. Granulomatous panniculitis in the setting of histoplasmosis in a patient with dermatomyositis on immunosuppressants. J Clin Images Med Case Rep. 2023; 4(10): 2665.
Introduction
Histoplasmosis is caused by the dimorphic fungus Histoplasma capsulatum which is found worldwide, but particularly in North and Central America [1]. Within the United States, it is most prevalent in the Southeast and Central regions and believed to favor temperate regions with specific soil features, such as acidity and organic content [2,3,4]. In endemic areas, over half of adults have been infected through inhalation of spores followed by hematogenous dissemination by macrophages traveling via lymphatics and the reticuloendothelial system [3,4,5]. Infection is usually asymptomatic but can result in severe illness, and among endemic mycoses, histoplasmosis is the most common cause for hospitalization [6]. Cardinal features of infection include pulmonary infiltrates, oral ulcers, lymphadenopathy, and hepatosplenomegaly. Skin lesions have been reported in 10 to 15 percent of cases of disseminated histoplasmosis, and characteristic lesions include nodules, ulcers, vesicles, and abscesses [1-7].
Panniculitis is an inflammatory disease that specifically targets the subcutaneous fat, usually presenting with erythema and inflammatory nodules or plaques below the dermis [1]. Depending on the type of panniculitis, features such as Ulceration, atrophy, or sclerosis may also be present. With regard to infectious panniculitis, it usually presents as a lobular panniculitis-i.e., a later-stage lesion in contrast to early-stage septal panniculitis-caused by bacterial, mycobacterial, fungal, protozoal, or viral infections [8]. Infection may occur due to hematogenous dissemination, contiguous spread, or direct inoculation. Streptococcus is frequently encountered as an infectious agent causing panniculitis, especially in children, with other agents including Epstein-Barr virus, Cytomegalovirus, Yersinia spp., mycoplasma, chlamydia, histoplasma and coccidioides [9]. Further, Patients on immunosuppressive therapy are at increased risk for infectious panniculitis and/or disseminated endemic mycoses [3,4].
Case report
An 83-year-old female, with a past medical history of amyopathic dermatomyositis with myositis-specific autoantibodies positive for TIF1-ϒ, atrial fibrillation, and hypertension presented to her local emergency department with a dime-sized rash on her right medial thigh, which was diagnosed as cellulitis. She was discharged with a prescription for cephalexin and doxycycline. One week later, the patient presented to a second outside hospital with worsening of her right medial thigh rash and was treated with intravenous vancomycin and discharged with linezolid. The following week, the patient returned to the initial hospital with an expanding, tender and purplish rash to the thigh, reporting that the symptoms and size of the rash had increased, despite adhering to prescribed antibiotics. The patient also reported fever and chills, but otherwise review of systems was negative. Of note, she denied muscle weakness or dysphagia, as well as joint pain, swelling or stiffness. Notably, on history-taking it was elicited that the patient emigrated from Colombia many years ago and lived in South Florida before moving to New Jersey two years prior; in addition, she reported being a keen gardener.
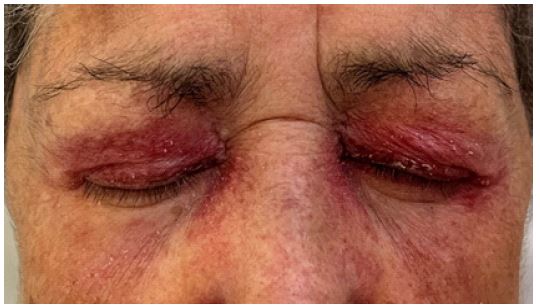
On physical examination, she was noted to have a violaceous indurated tender plaque covering the entire right medial thigh with satellite nodules (shown in Figure 1). Skin examination also revealed a heliotrope rash on her eyelids (shown in Figure 2) and shawl sign over the patient’s chest. Venous doppler was negative for deep or superficial venous thrombosis bilaterally. Computed Tomography (CT) of the chest, abdomen and pelvis did not reveal infiltrates, consolidations, malignancy, or lymphadenopathy. She was admitted to the hospital due to concern for a dermatomyositis flare and cellulitis refractory to multiple outpatient antibiotic therapies. On admission, the patient was taking prednisone 20 mg daily and mycophenolate 500 mg BID, In addition to rituximab therapy every six months with her last infusion three weeks prior. She was also treated earlier that year with monthly intravenous immunoglobulin infusions due to an unresolved dermatomyositis rash. The patient was up-to-date with annual mammography, but had no recent colonoscopy screenings.

The patient’s treatment plan initially involved administering intravenous vancomycin and ceftazidime. Two punch biopsies were performed on the center of the plaque, along with two additional biopsies performed on the satellite lesions. The pathology on the tissue revealed granulomatous lobular necrotizing panniculitis with vascular thrombosis, and superimposed features of chronic lymphedema. This granulomatous inflammation with mild lymphocytic cell infiltrate in the subcutis had features that could represent a paradoxical granulomatous eruption due to rituximab therapy. Initial acid-fast bacteria, periodic acid-schiff and gram stains were negative. Two of the biopsy specimens collected were sent for tissue analysis, including bacterial, fungal, and acid-fast bacilli smear and culture. Given the initial absence of infectious pathology, the patient was started on high dose steroids (prednisone 80 mg) along with trime thoprim-sulfamethoxazole for pneumocystis jirovecii pneumonia prophylaxis. The patient’s plaques on the right thigh improved during her hospitalization, leading to follow-up scheduled with her outpatient rheumatologist.
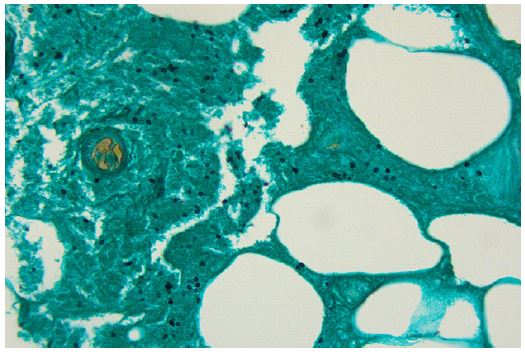
Twenty-three days after the initial tissue cultures, results returned positive for mold, ultimately identifying histoplasmosis growth. H. galactomannan urine antigen test was ordered and was elevated. Additionally, a Grocott Methenamine Silver (GMS) stain was performed on the original slides, which showed round to ovoid yeast-type forms with some budding forms in necrotic areas (Figure 3). Throughout this period, the patient’s thigh plaques continued to improve without antifungal therapy. However, due to the positive urine antigen and tissue culture results, the patient was started on posaconazole and her immunosuppressants decreased. She is currently being monitored with outpatient follow-up appointments in infectious disease, rheumatology, and dermatology.
Discussion
Reaching a diagnosis of an infectious etiology was complicated by the patient’s past medical history and clinical presentation and her response to immunosuppression. Indeed, connective tissue disorders and histoplasmosis share overlapping clinical findings, including erythematous indurated skin plaques, pulmonary infiltrates, myalgias, erythema nodosum, and lymphadenopathies. Half of patients with rheumatologic syndromes exhibit septal panniculitis, which is characterized by inflammation of the subcutaneous fat [2]. In the context of an infection, an inflammatory response can be misinterpreted as a manifestation of the patient’s underlying rheumatological disease, rather than a direct consequence of microorganisms. As such, histoplasmosis can be misdiagnosed as a dermatomyositis flare, as was a suspicion in this case. Here, the patient’s inflammatory response showed clinical improvement on increased steroids. Given the challenging nature of treating dermatomyositis, especially in those manifesting clear evidence of active disease, an infectious diagnosis was considered, albeit lower on our list of possibilities until ruled out. While the immunocompromised status of HIV and malignancy patients instinctively guides clinicians to root out infectious etiologies, rheumatology patients on immunosuppressants have similarly high immunocompromised burdens and also deserve a thorough workup for infectious diseases. In the case of this dermatomyositis patient receiving a significant immunosuppressive regimen, the necessity of tissue culture was imperative. Her treatment significantly increased the risk of opportunistic infections, masking (or concealing) them as manifestations of her underlying connective tissue disease. In one study, 26-50% of patients with myositis or systemic lupus erythematosus faced complications associated with infections and the frequent use of immunosuppressive agents, such as prednisone, greatly increased the risk of infection [10]. In fact, the myositis group in this study had the highest incidence rate of opportunistic infections when compared to other systemic rheumatic diseases.
Further complicating the patient’s diagnosis is that skin lesions are relatively uncommon in histoplasmosis except in patients with advanced HIV, Where they are seen more frequently [4,11]. Panniculitis has been described as an unusual form of presentation in histoplasmosis, whose lesions are usually mucocutaneous, primarily found in the oropharynx beginning as flat, non-tender plaques or nodules that evolve into painful ulcerations [7,11]. Nevertheless, cases have been reported with skin findings from erysipelas-like plaques to subcutaneous, erythema nodosum-like nodules [11]. Review of literature reveals some previous case reports of histoplasma panniculitis, and a common factor in most of these cases is that the patients were immunocompromised, usually due to immunosuppressive therapy with medications including prednisone and mycophenolate [1,5,7,12,13]. In addition, there are also case reports of histoplasmosis associated with rituximab therapy [5,14].
Recommendations for histoplasmosis treatment differ based on the affected location, severity of disease, and immunocompromised state of the host. Infectious diseases society of America guidelines from 2007 propose the use of amphotericin B deoxycholate (two-four weeks) followed by itraconazole (three months) for disseminated histoplasmosis [15]. In 2016, a study was published comparing itraconazole to posaconazole for the treatment of histoplasmosis, finding that posaconazole yielded a reduced length of treatment and no significant side effects. Accordingly, posaconazole is considered a suitable alternative for management [16]. Of the options available to the patient, posaconazole therapy was preferred due to its ease of administration, proven in vitro efficacy, and reduced side effect profile.
In short, inflammatory infiltrates of fungal infections can mimic many other pathologies both clinically and histologically. As histoplasmosis infections in general respond well to antifungal therapies [2,3,12], keeping a broad differential in mind is crucial when approaching patients on immunosuppressants to reach an accurate diagnosis and avoid delays in treatment.
Conclusion
This case underscores the importance of expanding the list of differentials to include infectious sources when clinically encountering atypical presentations in patients on immunosuppressive therapy. Panniculitis in patients with dermatomyositis on immunosuppressants is one such case where clinicians must have a high degree of suspicion to exclude an infectious etiology. To achieve a definitive diagnosis, it becomes imperative to conduct appropriate tests, such as biopsy and tissue culture sampling.
Declarations
Patient consent: Written informed consent was obtained from the patient for publication of this case report and any accompanying images.
Conflict of interest: The authors have no conflicts of interest to declare.
Author contributions: Each of the six authors of this case report provided substantial contributions to its conception and drafting, exercised final approval of the version to be published, nd agree to be accountable for all aspects of the work.
References
- Sawalha AH, Lutz BD, Chaudhary NA, Kern W, Harley JB, Greenfield RA. Panniculitis: a presenting manifestation of disseminated histoplasmosis in a patient with rheumatoid arthritis. J Clin Rheumatol. 2003; 9(4): 259-262.
- Ceccato F, Gongora V, Zunino A, Roverano S, Paira S. Unusual manifestation of histoplasmosis in connective tissue diseases. Clin Rheumatol. 2007; 26(10): 1717-1719.
- Chang P, Rodas C. Skin lesions in histoplasmosis. Clinics in Dermatol. 2012; 30: 592-598.
- Kauffman C. Pathogenesis and clinical manifestations of disseminated histoplasmosis. In: UpToDate, Post TW (Ed.), UpToDate, Waltham, MA. 2023.
- Quinter S, Cheng C, Prakash N, Currie G, Fleming M. Disseminated histoplasmosis presenting as panniculitis in two immunosuppressed patients. Dermatol Online J. 2012; 18(11): 3.
- Chu JH, Feudtner C, Heydon K, Walsh TJ, Zaourtis TE. Hospitalization for endemic mycoses a population-based national study. Clin Infect. 2006; 42: 822-825.
- Flores-Bozo LR, Ortiz-Brizuela E, Soto-Ramírez LE. Histoplasma panniculitis in a patient with systemic lupus erythematosus. An Bras Dermatol. 2019; 94(1): 96-98.
- Requena L, Sánchez YE. Panniculitis. Part II. Mostly lobular panniculitis. J Am Acad Dermatol. 2001; 45(3): 325-361.
- Morita TCAB, Trés GFS, García MSC, Halpern I, Criado PR, Freire de Carvalho J. Panniculitides of particular interest to the rheumatologist. Adv Rheumatol 2019; 59(35).
- Hsu CY, Ko CH, Wang JL, Hsu TC, Lin CY. Comparing the burdens of opportunistic infections among patients with systemic rheumatic diseases a nationally representative cohort study. Arthritis Res Ther. 2019; 21(1): 211.
- BCohen PR, Bank DE, Silvers DN, Grossman ME. Cutaneous lesions of disseminated histoplasmosis in human immunodeficiency virus-infected patients. J Am Acad Dermatol. 1990; 23(3 Pt 1): 422-428.
- Huston JW 3rd, McNabb PC 2nd, Frias JP. Histoplasma panniculitis in dermatomyositis. J Clin Rheumatol. 1997; 3(6): 353-357.
- Dufresne SF, LeBlanc RE, Zhang SX, Marr KA, Neofytos D. Histoplasmosis and subcutaneous nodules in a kidney transplant recipient versus fungal panniculitis. 2013; 15(20): E58-E63.
- Vigna-Perez M, Hernández-Castro B, Paredes-Saharopulos O, et al. Clinical and immunological effects of Rituximab in patients with lupus nephritis refractory to conventional therapy a pilot study. 2006; 8(3): R83.
- Wheat LJ, Freifeld AG, Kleiman MB, et al. Clinical practice guidelines for the management of patients with histoplasmosis Update by the Infectious Diseases Society of America. 2007 Oct; 45(7): 807-825.
- Krishna B, Akram S, Sundareshan V, et al. Comparison of Posaconazole and Itraconazole for treatment of histoplasmosis. 2016; 3(1): 16-46.