
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
A case of pancreatic neuroendocrine carcinoma was diagnosed based on the dramatic changes observed in imaging over a two-month period
Masami Miki1*; Makoto Hara1; Kenya Akagi1; Yasuhiro Komori2; Keijiro Ueda2; Nao Fujimori2; Shuji Matsuura3; Seiya Momosaki4; Toyoma Kaku1; Yoshihiro Ogawa2
1Department of Gastroenterology, NHO Kyushu Medical Center, Fukuoka, Japan.
2Department of Medicine and Bioregulatory Science, Graduate School of Medical Sciences, Kyushu University, Fukuoka, Japan.
3Department of Radiology, NHO Kyushu medical center, Fukuoka, Japan.
4Department of Pathology, NHO Kyushu medical center, Fukuoka, Japan.
*Corresponding Author : Masami Miki
Department of Gastroenterology, NHO Kyushu Medical Center, 1-8-1 Jigyohama Chuo-ku, Fukuoka City Fukuoka, Japan.
Tel: +81-92-852-0700;
Email: ma-sya.meteor@kdp.biglobe.ne.jp
Received : Sep 27, 2023
Accepted : Oct 24, 2023
Published : Oct 31, 2023
Archived : www.jcimcr.org
Copyright : © Miki M (2023).
Abstract
Pancreatic Neuroendocrine Carcinoma (PanNEC) is a rare type of cancer with rapid progression and a poor prognosis. In this report, we present a case of PanNEC that was diagnosed after a dramatic change in its imaging features. A 73-year-old woman with upper abdominal pain was referred to our hospital for evaluation of a 28 mm cystic mass found on abdominal computed tomography. The tumor was also visualized as a cyst on endoscopic ultrasound and did not enhance, but it compressed the main pancreatic duct. Two months later, the tumor had increased in size (50 mm) and transformed into a solid lesion. Pathological findings from a specimen obtained by EUS-FNA revealed that the tumor was PanNEC with a Ki-67 index of >80%. The patient’s survival time was only 4 months after the onset. In considering a case of an uncommon pancreatic mass, it’s important to bear in mind the possibility that it could be PanNEC.
Keywords: Pancreatic neuroendocrine carcinoma (PanNEC); Cystic component; Pancreatic cyst; Obstructive pancreatitis.
Citation: Miki M, Hara M, Akagi K, Komori Y, Ueda K, et al. A case of pancreatic neuroendocrine carcinoma was diagnosed based on the dramatic changes observed in imaging over a two-month period. J Clin Images Med Case Rep. 2023; 4(10): 2666.
Introduction
Pancreatic neuroendocrine neoplasm (PanNEN) is a rare disease, with an overall prevalence of ≤5 per 100,000 people. PanNENs are classified into pancreatic neuroendocrine tumor (PanNET) Grade 1,2 and 3, and pancreatic neuroendocrine carcinoma (PanNEC) based on tumor differentiation [1]. Among PanNENs, PanNEC, defined as the most poorly differentiated tumor, accounts for only 7.5% [2]. PanNEC is known for its rapid progression and poor prognosis. In most cases, PanNEC tumors are already large or have metastasized to distant organs when they are detected during imaging examinations. However, some cases have been reported as relatively small tumors without metastases, making them difficult to diagnose through imaging modalities such as CT and MRCP. Therefore, histological examination using Endoscopic Ultrasound (EUS) guided Fine-Needle Aspiration (FNA) plays a crucial role in achieving an accurate diagnosis [3]. The diagnosis of PanNEN is considerably challenging in cases where EUS-FNA cannot be performed for various reasons.
Case presentation
A 73-year-old Japanese woman was referred to our hospital for further evaluation of upper abdominal pain that had started two weeks prior. Her laboratory results showed a high white blood cell count (9000/μL) and elevated amylase levels (856 U/L). CA19-9 (9 IU/mL) and CEA (3 ng/mL) were within normal limits. Abdominal computed tomography (Figure 1a) revealed a cystic mass in the pancreatic head measuring 28 mm in size and dilatation of the upstream Main Pancreatic Duct (MPD) with a diameter of 5 mm. On Magnetic Resonance Imaging (MRI), the cystic mass exhibited mild signal intensity on T2-weighted images (Figure 1b). In Diffusion-Weighted Imaging (DWI), the mass displayed high signal intensity (Figure 1c).
Endoscopic ultrasound (EUS) (Figure 1d) detected the lesion as a cystic area with several septa, and Contrast-Enhanced EUS (CE-EUS) showed no enhancement inside the lesion. Therefore, we did not perform EUS-FNA. Endoscopic Retrograde Pancreatography (ERP) (Figure 1e) revealed MPD stenosis, which appeared to be caused by compression from the mass. There was no communication between the cystic mass and the pancreatic duct. The cytology of the pancreatic juice did not indicate malignancy. Several days later, her abdominal symptoms naturally improved, and she was discharged.
However, abdominal pain recurred, and she was readmitted to our hospital 2 months after the onset. A CT scan during the second admission (Figure 2a) showed that the lesion in the pancreatic head had turned into a solid tumor, and it had increased in size. The dilatation of the MPD had worsened, and serum amylase levels were elevated, indicating obstructive pancreatitis.Additionally, the CT scan revealed a solid component in the portal vein, which appeared to be a tumor thrombus (Figure 2b).
We inserted an endoscopic pancreatic stent (EPS) because the MPD dilatation had worsened, as indicated by ERP findings (Figure 2c). Additionally, we performed an EUS-FNA to diagnose the solid tumor (Figure 2d), which had previously presented as a cystic lesion. Histopathological examination of the FNA specimen revealed irregularly arranged small tumor cells with round nuclei and a high nucleus-to-cytoplasm ratio (Figure 3a, 3b). Immunohistochemistry demonstrated that the Ki-67 labeling index of the pancreatic tumor was ≥80% (Figure 3c). Immunohistochemical examination of the tumor cells showed positivity for chromogranin A and synaptophysin. Overexpression of p53 was also observed.
Fluorodeoxyglucose positron emission tomography (FDG-PET) showed abnormal uptake only in the pancreatic lesion (standardized uptake values: SUV max early 13.48, delay 17.73) (Figure 4-a). Somatostatin receptor scintigraphy (SRS) showed no abnormal uptake (Figure 4-b). The NSE (15.4 ng/mL) slightly exceeded the upper limit (47 ng/mL, 15.1 ng/mL).
The tumor was diagnosed as a PanNEC according to the World Health Organization (WHO) classification of endocrine tumors [4]. She was administered etoposide and cisplatin as first-line chemotherapy. However, her performance status worsened during the first course of chemotherapy. Finally, she passed away due to chemotherapy-induced febrile neutropenia only 4 months after the onset.

A. Computed tomography (CT) image showed cystic lesion in the pancreatic head (arrow) and dilatation of the upstream main pancreatic duct (MPD) (arrow-head).
B. Magnetic resonance imaging (MRI) revealed the lesion with mild signal intensity in the head of Pancreas (arrow).
C. The lesion exhibited high signal intensity on diffusion-weighted imaging (DWI) (arrow).
D. The pancreatic anechoic mass was not enhanced on contrast-enhanced endoscopic ultrasound (arrow).
E. Endoscopic retrograde cholangiopancreatography revealed MPD stricture of pancreatic head (arrow-head).
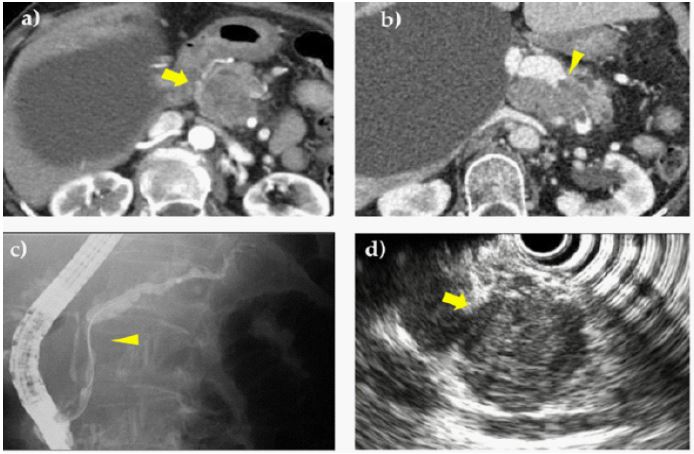
A. CT revealed that the tumors became mildly enhanced and solid with increased in size (arrow).
B. CT indicated tumor thrombus in the portal vein (allow-head).
C. ERP showed that MPD stricture worsened (arrow-head).
D. EUS showed the mass as a hypo-echoic lesion (arrow).
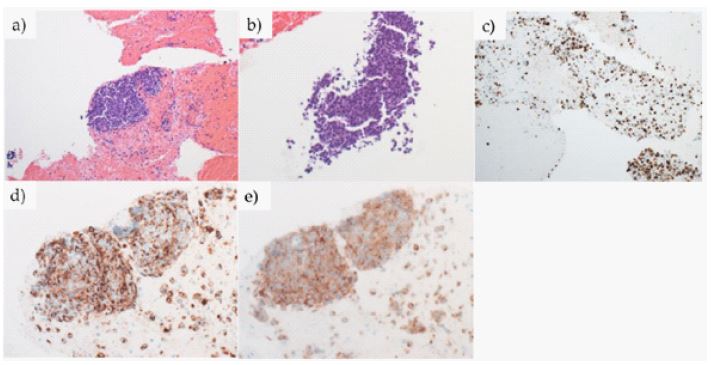
C. Immunohistochemistry showed that Ki-67 labeling index of pancreatic tumpr is 80% (MIB-1, stain. original magnification 100x).
D. Immunohistochemistry showed positive staining for chromogranin A (d, original magnification 100x).
E. Synaptophysin (e, original magnification 100x).
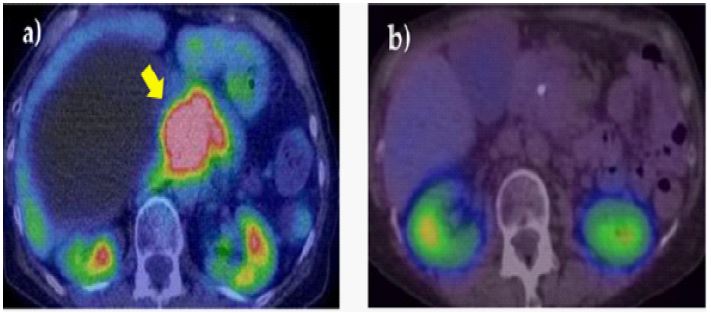
B. Somatostatin receptor scintigraphy (SRS) showed no abnormal intake.
Discussion
Here, we report a case of PanNEC that was initially identified as a cyst and was diagnosed after it transformed into a tumor. The patient’s survival time after onset was only 4 months.
In the initial imaging findings, the compression of the main pancreatic duct and the irregular shape of the cystic mass suggested the possibility of malignancy in the tumor. However, we were unable to make an accurate diagnosis during the initial admission.
Typically, PanNENs manifest as hyper-vascular lesions with a solid and round shape on contrast-enhanced CT scans [5], and some PanNENs are known to exhibit cystic lesions [6]. A meta-analysis has indicated that the presence of cystic components in PanNENs suggest an indolent biological behavior, as it is associated with a better prognosis compared to PanNENs without cystic lesions [7]. In another study, it was found that while 7% of PanNET G1/2 had cystic area in more than 90% of the tumor, this feature was not observed in PanNECs [8].
The presence of cystic features in this case not only made it challenging to distinguish PanNEC from other potential diagnoses but also presented difficulties in performing EUS-FNA. It is worth noting that the complication rate associated with EUS-FNA for pancreatic cystic lesions has been reported to be higher than that for pancreatic solid lesions [9]. In Japan, unlike in other countries, EUS-FNA has rarely been carried out for cystic lesions due to concerns about potential dissemination, as well as the risks of complications such as pancreatitis and infection [10]. Performing EUS-FNA during the initial admission might have contributed to a more accurate and earlier diagnosis. When encountering a pancreatic mass with unusual features, it is indeed important to reconsider the indication for EUS-FNA carefully.
The cystic lesion increased in size and transformed into a solid mass in just 2 months. Furthermore, the presence of tumor thrombosis in the portal vein prompted us to reach a conclusion regarding the tumor. Finally, she was diagnosed with PanNEC with the Ki-67 index ≥80% by histological examination with EUS-FNA.
Although regimen of etoposide and cisplatin [11], which is a standard first-line therapy option for PanNEC wasadministered immediately after the diagnosis, she died after just 1 month.
Conclusion
Herein, we report a case of PanNEC with an unusual initial imaging finding, presenting as a cyst. The diagnosis was made after the transformation into a solid tumor through pathological examination with EUS-FNA. When encountering a case of uncommon pancreatic mass, we should consider the possibility that it may be PanNEC. Given the aggressive nature of this disease, there is a need for consensus on early diagnostic methods for PanNEC.
Acknowledgements: None.
References
- WHO Classifcation of Tumours Editorial Board. WHO classifcation of endocrine and neuroendocrine tumours. 2022.
- Ito T, Igarashi H, Kazuhiko K, Sasano H, Okusaka T, et al. Epidemiological trends of pancreatic and gastrointestinal neuroendocrine tumors in Japan: a nationwide survey analysis. J Gastroenterol. 2015; 50: 58-64.
- Lee L, Ito T, Jensen RT. Imaging of pancreatic neuroendocrine tumors: recent advances, current status, and controversies. Expert Rev Anticancer Ther. 2018; 18: 837-60.
- Rindi G, Mete O, Uccella S, Basturk O, La Rosa S, et al. Overview of the 2022 WHO Classification of Neuroendocrine Neoplasms. Endocr Pathol. 2022; 33: 115-54.
- La Salvia A, Persano I, Parlagreco E, Audisio A, Cani M, et al. Pancreatic adenocarcinoma and pancreatic high-grade neuroendocrine carcinoma: two sides of the moon. Medical Oncology. 2022; 39.
- Goh BKP, Ooi LLPJ, Tan YM, Cheow PC, Chung YFA, et al. Clinico-pathological features of cystic pancreatic endocrine neoplasms and a comparison with their solid counterparts. European Journal of Surgical Oncology. 2006; 32: 553-6.
- Zhu J kang, Wu D, Xu J wei, Huang X, Jiang Y yuan, Edil BH, et al. Cystic pancreatic neuroendocrine tumors: A distinctive subgroup with indolent biological behavior? A systematic review and meta-analysis. Pancreatology. 2019; 19: 738-50.
- Kim DW, Kim HJ, Kim KW, Byun JH, Song KB, et al. Neuroendocrine neoplasms of the pancreas at dynamic enhanced CT: Comparison between grade 3 neuroendocrine carcinoma and grade 1/2 neuroendocrine tumour. Eur Radiol. 2015; 25: 1375-83.
- Wang KX, Ben QW, Jin ZD, Du YQ, Zou DW, et al. Assessment of morbidity and mortality associated with EUS-guided FNA: A systematic review. Gastrointest Endosc 2011; 73: 283-90.
- Nakai Y, Isayama H, Itoi T, Yamamoto N, Kogure H, et al. Role of endoscopic ultrasonography in pancreatic cystic neoplasms: Where do we stand and where will we go? Digestive Endoscopy. 2014; 26: 135-43.
- Morizane C, Machida N, Honma Y, Okusaka T, Boku N, et al. Effectiveness of Etoposide and Cisplatin vs Irinotecan and Cisplatin Therapy for Patients with Advanced Neuroendocrine Carcinoma of the Digestive System: The TOPIC-NEC Phase 3 Randomized Clinical Trial. JAMA Oncol. 2022; 8: 1447-55.