
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 4
Epicardial lipomatosis; An unexpected finding
Danay Pérez Mijenes*; João Caiano Gil
Internal Medicine Department, Pedro Hispano Hospital, Matosinhos Local Health Unit, Senhora da Hora, Portugal.
*Corresponding Author : Danay Pérez Mijenes
Internal Medicine Department, Pedro Hispano Hospital, Matosinhos Local Health Unit, Senhora da Hora, Portugal.
Email: danaypm@yahoo.es
Received : Sep 06, 2023
Accepted : Oct 25, 2023
Published : Nov 01, 2023
Archived : www.jcimcr.org
Copyright : © Mijenes DP (2023).
Citation: Mijenes DP, Gil JC. Epicardial lipomatosis; An unexpected finding. J Clin Images Med Case Rep. 2023; 4(11): 2668.
Clinical image description
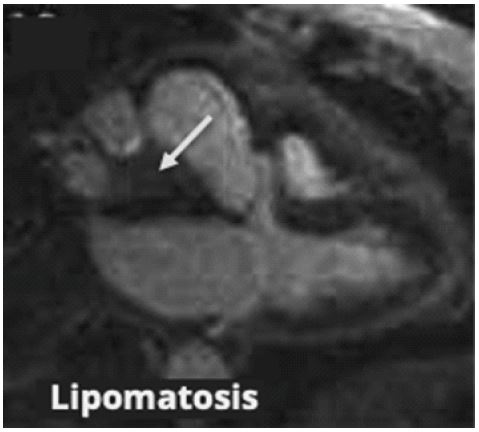
A 75-year-old female patient with hypertension, obesity, and dyslipidemia is being followed up in primary health care. She was referred to the hospital due to the finding on transthoracic echocardiography of a 55x30 mm dense, oval image at the level of the right atrium in relation to the interauricular septum. A transesophageal echocardiogram (TEE) confirmed above findings, suggesting a lesion of similar size, whose origin seemed to be centered on the interauricular septum, with no evidence of obstruction to blood flow at its location.
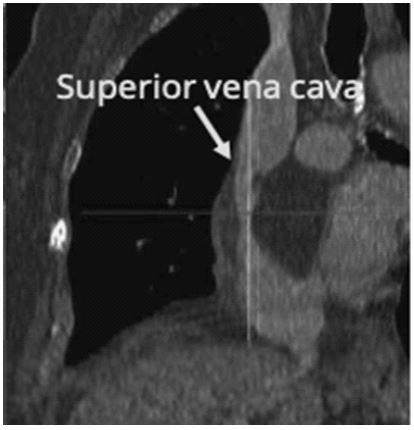
The investigation continued with computed tomography angiography (CTA) and cardiac magnetic resonance imaging (CMR), revealing an epicardial lipomatosis extending along the posterior surface of the right atrium and the interauricular sulcus, of a lipid and non-vascularized nature, particularly marked at the level of the ostium of the superior vena cava, where it involves the vessel and seems to cause a partial reduction in its lumen. Due to the absence of signs and symptoms, there were no criteria for urgent cardiac surgery, the patient was referred to the cardiothoracic surgery outpatient clinic for follow-up.
Epicardial lipomatosis (EL) is a rare disease characterized by greater development of this layer of adipose tissue due to adipocyte hyperplasia [1,4]. Its etiology is unclear, but it seems to predominate in older, obese people [2-4], and preferentially in women [3]. Its echocardiographic appearance can lead to misdiagnosis due to its similarity to other pathologies, and CMR is an essential test for the correct identification of this entity [1].
In this case, CMR allowed us not only to clarify the features of the lesion, but also to identify the luminal obstruction of the superior vena cava, which could not be seen on TEE and which could be crucial for the subsequent therapeutic approach.

References
- Magalhães P, Bettencourt N, Sampaio F, Carvalho S, Moreira JI, Gama V. What doesn’t kill you makes you fat!. Rev Port Cardiol. 2015; 34(4): 295-6.
- Laura DM, Donnino R, Kim EE, Benenstein R, Freedberg RS, Saric M. Lipomatous Atrial Septal Hypertrophy: A Review of Its Anatomy, Pathophysiology, Multimodality Imaging, and Relevance to Percutaneous Interventions. J Am Soc Echocardiogr. 2016; 29(8): 717-723.
- Pugliatti P, Patanè S, De Gregorio C, Recupero A, Carerj S, Coglitore S. Lipomatous hypertrophy of the interatrial septum. Int J Cardiol. 2008; 130(2): 294-5.
- Bertaso AG, Bertol D, Duncan BB, Foppa M. Epicardial Fat: Definition, Measurements and Systematic Review of Main Outcomes. Arq Bras Cardiol. 2013; 101(1): e18-28.