
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Research Article - Open Access, Volume 4
Effects of cardiopulmonary and metabolic rehabilitation in post-COVID-19 patients: Clinical trial
Bruno Tagliapietra Canabarro¹#; Marina André Remour¹#; Taís Flôres de Oliveira¹; Raphael Boesche Guimarães1; Maria Claudia Irigoyen1,2; Vinicius Serra Peringer1; Bruna Eibel¹*
1Institute of Cardiology/Fundação Universitária de Cardiologia (IC/FUC), Porto Alegre/RS, Brazil.
2Heart Institute (InCor) HC-FMUSP, São Paulo/SP, Brazil.
#The Authors Contributed Equally.
*Corresponding Author : Bruna Eibel
Institute of Cardiology/Fundação Universitária de Cardiologia (IC/FUC), Porto Alegre/RS, Brazil.
Email: brunaeibeil@gmail.com
Received : Sep 20, 2023
Accepted : Oct 26, 2023
Published : Nov 02, 2023
Archived : www.jcimcr.org
Copyright : © Eibel B (2023).
Abstract
Objective: To evaluate the effects of cardiopulmonary rehabilitation on the functional capacity of post-COVID-19 individuals.
Methods: Clinical trial, 7 patients participated in the study who tested positive for COVID-19. Participants underwent a 30-session rehabilitation program. They were evaluated using: Post COVID-19 Functional Scale (PCFS), inspiratory and expiratory muscle strength, 6-minute walk test (6MWT), 30-second sit-to-stand test (SE30’), hand grip (HG), VO2max, maximum HR, resting and reserve. Functional variables were analyzed using ANOVA for repeated measures and the Bonferroni multiple comparison test, considering a significance level of 5%.
Results: The participants showed improvement in their functional status, with a decrease in the PCFS score (p=0.006), improvement in MIP (p=0.013), distance covered in the 6MWT (p=0.022), HGSR (p=0.005) and HGSL (p=0.009). In SE30’, they showed improvement in the intermediate (p=0.002) and final (p=0.046) assessments.
Conclusions: The individuals demonstrated a decrease in functional limitations, improvement in functional capacity, inspiratory and lower limb muscle strength, handgrip strength after the 7th week of rehabilitation, with maintenance of the functional status being promoted until the end of the program. Implying the reestablishment of the global functional state of the pa-tients.
Keywords: Rehabilitation; Acute COVID-19 syndrome; Functional status; Physical therapy specialty.
Citation: Canabarro BT, Remour MA, de Oliveira TF, Guimarães RB, Eibel B, et al. Effects of cardiopulmonary and metabolic rehabilitation in post-COVID-19 patients: Clinical trial. J Clin Images Med Case Rep. 2023; 4(11): 2670.
Introduction
The new coronavirus, SARS-CoV-2, emerged in December 2019, SARS-CoV-2, expanded throughout China, soon after reaching worldwide proportions [1,2]. It is a virus with high transmissibility [3,4] and an estimated mortality rate of approximately 3.7% [3,5].
Most COVID-19 infections are mild, but they can be severe or critical, causing dyspnea, hypoxemia, severe lung damage, respiratory failure, septic shock, and multiple organ failure [6-8], requiring oxygen supplementary and prolonged mechanical ventila-tion [9]. The presence of comorbidities such as Chronic Obstructive Pulmonary Disease (COPD), asthma, heart disease, cerebrovascular disease, diabetes, kidney failure and cancer are associated with a worse prognosis and longer hospital stay [10,11].
People who need prolonged hospitalization are more susceptible to developing muscle weakness acquired in the ICU [12,13], loss of muscle function and decreased functional capacity [14], diaphragmatic muscle weakness, decreased lung compliance [15,16], developing the critically ill polyneuromyopathy syndrome (CDP) [17], impacting on the decrease in quality of life [18].
Complications arising from COVID-19 in the lung tissue such as fibrosis, consolidation, vascular thickening, pleural effusion, bronchiectasis can occur in most patients [15]. These seem to be prone to movement-related fatigue, similar to patients with ARDS, even those who do not develop critical illness [17].
Previous studies have shown that post-COVID-19 rehabilitation, involving aerobic and resistance exercises, combined with respiratory muscle training, is able to improve functional capacity [19], peripheral muscle strength [20], respiratory function and quality of life [21] in individuals affected by the disease. Therefore, rehabilitation following SARS-CoV-2 infection is an essential component of the care plan for this population [22].
However, there is a lack of evidence regarding outpatient rehabilitation after COVID-19. Thus, the present study aimed to evalu-ate the effects of cardiopulmonary and metabolic rehabilitation on the functional capacity of post-COVID-19 individuals.
Materials and methods
This is a clinical trial, in which a sample of individuals after infection with the SARS-CoV-2 virus was included. To participate in the study, individuals should be over 18 years of age, of both sexes, and present a positive RT-PCR or RT (rapid test) for COVID-19 in the last 4 months prior to inclusion (Figure 1). Participants were referred by partner health services. We considered the following exclusion criteria, patients who did not have a positive RT-PCR or TR, those with positive tests in a period longer than four months of inclusion, individuals with hemodynamic instability, physical limitations that prevented the performance of the initial evaluations, accident cerebrovascular disease, cancer and previous myocarditis. The present study was approved by the Ethics and Research Committee (CAAE 42014621.7.0000.5333) and the participants signed the informed consent form (TCLE).
The sample comprised 7 individuals (Table 1), who underwent a cardiopulmonary and metabolic rehabilitation program con-sisting of 30 sessions. The participants were submitted to a complete functional evaluation in 3 moments: Pre-participation, after 15 sessions and at the end of the program.
The assessment consisted of the Post-COVID-19 Functional Status Scale (PCFS), developed to monitor the course of symptoms and their impact on the functionality of patients infected with COVID-19 after hospital discharge. It has 6 levels: 0(no functional limitations), 1(insignificant functional limitations), 2(mild functional limitations), 3(moderate functional limitations), 4(severe functional limitations) and D(death). The scale was applied by a physiotherapist at baseline, intermediate and final assessments [23].
Functional capacity was measured by the six-minute walk test (6MWT). Performed in a corridor free of people, participants were instructed to walk at a fast pace for 6 minutes along a 30-meter course. Blood Pressure (BP), Heart Rate (HR), OxyOxygen Saturation (SpO2) and subjective effort scale for tiredness and dyspnea (modified BORG) were measured before and after the test. At the end of the test, the distance covered by the individual was checked and placed in the formula, which takes height, age and body weight into account, obtaining the normality parameter for each case [24].
Respiratory muscle strength, Maximal Inspiratory Pressure (MIP) and Maximal Expiratory Pressure (MEP) were assessed using a digital manovacuometer (MVD 300-U Homed). Both pressures were measured three times, obtaining a difference less than or equal to 10% between the 3 repetitions, interspersed with 2 minutes of rest, the highest value being considered. Between MIP and MEP measurements, there was a five-minute interval [25].
For Handgrip Strength (HGS), a handheld hydraulic dynamometer (Saehan-5001) was used. The test was performed with the individual sitting on a chair, with shoulders adducted, neutral rotation and elbow flexion at 90°, forearm in a neutral position holding the dynamometer and arm parallel to the body. From this position, the individuals were instructed to perform a maximum contraction during expiration. Three consecutive tests were performed and the average used as the HGS value. The test was performed on both limbs [26].
Indirect maximal oxygen consumption (VO2max) was measured using the Exercise Test (ET) on a treadmill (Inbrasport model ergometer) with a 12-lead electrocardiogram (Inbramed), using the Naughton protocol. The protocol starts with a treadmill speed of 1.0 miles per hour (mph) without incline, for warm-up purposes. Then go to 2.0 mph, maintaining zero elevation. From this stage, the speed is fixed at 2 mph and the ramp elevation is incremented by 3.5% every 3 minutes. HR, BP, SatO2, Borg pre and post test were evaluated [27].
The sessions were held at the Cardiopulmonary and Metabolic Rehabilitation Center of the Institute of Cardiology/University Foundation of Cardiology (IC/FUC). Duration of 15 weeks, 2 sessions per week of 60 minutes each, totaling 30 sessions. HR, SpO2, BP and BORG were monitored in all sessions.
The rehabilitation protocol consisted of warm-up, respiratory muscle training, aerobic training, resistance training and stretching. The warm-up took place at the beginning of each session (stationary gait, shoulder flexion and extension, shoulder circumduction, trunk rotation, plantiflexion in orthostasis), consisting of 30 quick repetitions of each exercise.
Inspiratory Muscle Training (IMT) was performed shortly after warm-up. The POWERbreathe® inspiratory training device (POWERbreathe International Ltd., England, United Kingdom) was used. It consisted of five series of ten repetitions each, with a one-minute rest between each series. During training, patients were instructed to maintain diaphragmatic breathing. Subjects were submitted to IMT of moderate to high intensity, with an initial load set at 50% of MIP during the first two weeks, allowing for an adaptation period. Sequentially, load increases occurred at 55% MIP week 3, 60% MIP week 4, 65% MIP week 5, MIP 70% week 6, MIP 75% week 7, and MIP 80% of MIP in the 8th week. From weeks 9 to 15, load was adjusted weekly to maintain 80% MIP [28].
Aerobic training consisted of walking on a treadmill for 30 minutes, with a workload adjusted between 60%-80% of the maximum heart rate obtained through the exercise test.
Resistance muscle training consisted of 2 workouts: Workout A (extension/push exercises: diagonal abduction, machine bench press, rope triceps, leg extension, unilateral knee flexion, horizontal leg press and plantiflexion on the machine) and B (exercises of “pulling”/flexion: front pull, machine biceps, diagonal adduction, hip extension, squat, orthostasis plantiflexion and extension chair). All exercises were performed in 3 series of 10 repetitions and the load was adjusted weekly aiming at muscle fatigue in the last 3 repetitions.
At the end of each session, participants performed static stretching of lower and upper limbs, sustained for 30 seconds.
Statistical analysis
Data are presented as mean and standard deviation, and absolute frequency and percentage. For the analysis of the functional variables, the analysis for repeated measures (ANOVA) and the Bonferroni multiple comparison test were used. A significance level of 5% was used. The Statistical Package for the Social Sciences (SPSS) Windows v.22.0 program was used.
Considering an α=5% error and a power of 80%, the sample was calculated for 44 subjects, based on a previous study [34], tak-ing into account 10% of possible losses. The sample calculation was performed using the Winpepi program.
Results
Persistent post-COVID-19 sequelae at the time of assessment are described in Table 2. The results of the analyzed variables are shown in Table 3. Patients showed significant improvement in PCFS, when comparing baseline and final assessments. In the assessment of respiratory muscle strength, there was an improvement in MIP and MIP% from baseline to the intermediate as-sessment (7th week) and the mean was maintained after the final assessment (15 weeks). There were no differences in MEP and PE%.
In the measures of submaximal functional capacity evaluated by the 6MWT, the patients presented a greater distance covered and a higher percentage of the predicted distance when comparing the baseline and intermediate evaluations, with maintenance of the average values in the final evaluation, however, there was no difference for BORG fatigue and BORG dyspnoea.
The participants showed a significant improvement in lower limb strength, assessed by the 30’ sit-to-stand test, and handgrip strength in both limbs, when baseline and intermediate assessments were compared. In both tests, mean values were maintained at the time of the final evaluation. No difference was observed in any of the variables evaluated by the exercise test.
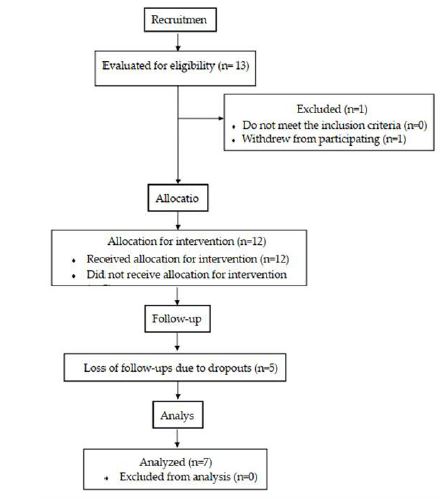
Table 1: Sample characteristics.
Variable |
N = 7 (%) |
|---|---|
Age(years) Sex Feminine Masculine Mass(kg) Height(cm) BMI(kg/m²) Comorbidities DM Obesity SAH Dyslipidemia Sedentarylifestyle Ischemicheart disease Hypothyroidism Hospitalization Needfor hospitalization Hospitalizationdays Ventilatorysupport NC NRRM HFNC NIV IMV Medicines Antihypertensive Anticoagulant |
53,2± 16,1* 3(42,8) 4(57,1) 75,6± 15,9* 162,4± 11,4* 28,4± 3,7* 2(28,6) 3 (42,8) 3 (42,8) 2 (28,6) 5 (71,4) 1 (14,3) 1 (14,3) 5(71,4) 14,7± 12,1* 3(42,8) 3(42,8) 1(14,3) 1(14,3) 0 2(28,6) 3(42,8) 1(14,3) |
Table 2: Post-COVID-19 sequelae.
Sequelae |
N = 7 (%) |
|---|---|
Fatigue/tiredness Dyspnea Headache Muscle pain Loss of hair Taste/smell loss Chest pain Dizziness Cough Palpitations Cepression/anxiety Difficulty with reasoning, language and memory |
5 (71,4) 1 (14,3) 0 1 (14,3) 3 (42,8) 3 (42,8) 1 (14,3) 0 2 (28,6) 0 6 (85,7) 3 (42,8) |
Table 3: Functional variables.
Assessment Moments |
||||
|---|---|---|---|---|
| First | Intermediate | last | p value | |
| PCFS | 1,9 ± 0,7 | 0,9 ± 0,7 | 0,6 ± 0,8 | 0,006† |
| Pimáx | 85,6 ± 31,2 | 113,4 ± 27,5 | 113,3 ± 40,9 | 0,013* |
| PI% | 83,6 ± 31,2 | 112,9 ± 18,9 | 113,3 ± 40,9 | 0,015* |
| PEmáx | 104,6 ± 44,1 | 127,4 ± 38,6 | 108,5 ± 31,3 | 0,227 |
| PE% | 100,0 ± 32,4 | 122,2 ± 31,1 | 105,8 ± 31,4 | 0,231 |
| 6MWT Dist(m) %pred BORGFpré BORGFpós BORGDpré BORGDpós |
464,1 ± 57,5 86,1 ± 18,7 0,3 ± 0,7 1,6 ± 3 1,4 ± 2,9 1,1 ± 1,7 |
539 ± 22,4 99,8 ± 15,2 0 0,2 ± 0,4 0,07 ± 0,2 0,1 ± 0,2 |
513,7 ± 40,6 95,7 ± 15,4 0 0,1 ± 0,2 0 0 |
0,022* 0,027* 0,397 0,207 0,246 0,099 |
| SE30’ (rep) | 10,2 ± 0,9 | 12,6 ± 0,8 | 12,1 ± 1,8 | 0,002*† |
| RHGS(kgf) | 27,3 ± 9,5 | 32,6 ± 7,7 | 32,9 ± 8,6 | 0,005* |
| LHGS(kgf) | 24,5 ± 9,9 | 31,2 ± 8,2 | >30,6 ± 8,7 | 0,009* |
| ET VO2max HRmax HRre HRres |
32,2 ± 7,7 135,7 ± 27,2 73,6 ± 15,6 67,6 ± 26,8 |
40,3 ± 4,9 146,7 ± 25,9 68,9 ± 9,5 77,9 ± 21 |
38 ± 10,5 135,6 ± 33,8 72 ± 21,8 63,6 ± 21,4 |
0,109 0,102 0,701 0,075 |
*: statistically significant between baseline and intermediate assessment, for p < 0.05. †: statistically significant between baseline and final assessment, for p< 0.05. Values are expressed as mean±SD. PCFS The Post COVID-19 functional status; PImax: maximum inspiratory pressure; PI%: % of predicted maximum inspiratory pressure; PEmax: maximum expiratory pressure; PE%: % of predicted maximum expiratory pressure; 6MWT: 6-minute walk test; Dist: distance from the 6MWT; BORGF: BORG scale muscle fatigue; BORGD: BORG scale dyspnea; SE30’: 30-second sit and stand test; RHGS: right hand grip strength; LHGS: left hand grip strength; ET: exercise test; VO2max: maximum oxygen volume; HRmax: maximum heart rate; HRre: resting heart rate; HRres: heart rate reserve. Significance level of p< 0.05.
Discussion
Our results demonstrate that individuals who underwent a cardiopulmonary and metabolic training program after COVID-19 infection improved their functional limitations, inspiratory muscle strength, lower limb muscle strength, and handgrip strength. However, this improvement was noticed in the intermediate evaluation and was not maintained until the final evaluation.
When applying the PCFS, we observed that our sample consisted of patients who went through different stages of disease severity. Hussein et al. [29], demonstrated that patients recovered from COVID-19 obtained fluctuating degrees of restrictions in their work-related, public and leisure activities or activities of daily living. Despite the heterogeneity and sample size, our study showed a significant improvement in the degree of functionality of patients recovered from COVID-19 who participated in a cardiopulmonary and metabolic rehabilitation program, starting from a mild to moderate degree of functionality to insignificant. Pant et al. [30], point out that the consequences on physical and mental health in post-COVID-19 patients need to be observed and that rehabilitation measures in post-acute care are essential.
Our findings are in line with the findings of Ahmed et al, who, through a pulmonary function test, demonstrated that the inspiratory muscle training performed obtained a significant improvement in the values of FVC% and FEV1%. In this study, the patients performed 2 daily sessions, 5 days a week, for 2 consecutive weeks with a threshold load of 50% of the maximum inspiratory pressure (MIP) [31]. In our study, we used a threshold of up to 85% of MIP using 5 sets with 10 repetitions and 60 seconds of rest between sets. The results in the inspiratory muscle training, mainly up to the 7th week, showed a significant increase, also reflecting in the improvement of the quality of life and functional capacity.
Kai Liu et al. [21] conducted a study with respiratory rehabilitation in post-COVID-19 patients for 6 weeks, 2 sessions per week and once a day for 10 minutes (at home). The authors observed that in the intervention group there was a significant improvement in the 6MWT distance and in the pulmonary function test. These findings corroborate ours and are compatible with the weeks of rehabilitation in which we obtained important differences in the global functional status. We can deduce that a smaller number of sessions combined with inspiratory muscle training is able to increase the functional capacity of patients recovered from COVID-19.
Despite the significant increase in the distance covered in the 6MWT, there was no difference in maximum VO2, maximum HR, reserve HR and resting HR. However, as shown in Table 3, we observed important clinical differences at all moments of maxi-mum VO2 evaluation. The non-difference can be explained by the low sample number.
Silva et al. [32] demonstrated that lower limb strength and aerobic resistance are associated with the practice of regular physical exercise, which is related to better performance in the sit-to-stand test and the 6MWT. In line with these findings, our study found that there was an improvement in performance when performing the sit-to-stand test at all times evaluated.
Del Brutto et al. [33] showed in their study a greater than 5% loss of handgrip strength after coronavirus infection, while Sansin et al [34] observed decreased handgrip strength in patients who required hospitalization, mainly among women. Results which suggest the musculoskeletal damage generated by SARS-CoV-2. Our program resulted in increases in handgrip strength by up to 27%, thus indicating improved overall muscle strength.
Even with limitations such as low adherence to cardiopulmo nary and metabolic rehabilitation, the number of patients who completed the program, the difficulty in recruiting patients to participate in the study and our rehabilitation center is not a reference for the treatment of COVID-19, our study was able to demonstrate that a program with a reduced number of sessions is safe and effective.
Therefore, we showed that a rehabilitation program for post-COVID-19 patients was able to provide functional improvements in these individuals from the 7th week onwards, with 15 sessions performed. We suggest that shorter duration programs be adopted aiming at greater adherence and segment of these patients. Given the brevity of the onset of the disease, more robust studies are needed to delve deeper into the effects of rehabilitation in this population.
Conclusion
Individuals post-COVID-19 infection, submitted to a 15-week rehabilitation program, demonstrated improvement in functional limitations after the end of the program. They showed improvement in functional capacity, inspiratory muscle strength, lower limb muscle strength and handgrip strength after the 7th week of treatment, maintaining the functional state until the end of the proposed program. Due to the large number of dropouts during follow-up, we believe that a program of 15 sessions lasting 7 weeks is sufficient for the functional recovery of these patients.
Declarations
Funding: This research received no external funding.
Informed consent statement: Informed consent was obtained from all subjects involved in the study.
Conflicts of interest: The authors declare no conflict of interest.
References
- Lipsitch M, Swerdlow DL, Finelli L. Defining the Epidemiology of Covid-19-Studies Needed. N Engl J Med. 2020; 382: 1194-6.
- Purcell LN, Charles AG. An Invited Commentary on “World Health Organization declares global emergency: A review of the 2019 novel Coronavirus (COVID-19)”: Emergency or new reality? Int J Surg. 2020; 76: 111.
- Khachfe HH, Chahrour M, Sammouri J, Salhab HA, Makki BE, et al. An Epidemiological Study on COVID-19: A Rap-idly Spreading Disease. Cureus . 2020; 12.
- Wilder-Smith A, Chiew CJ, Lee VJ. Can we contain the COVID-19 outbreak with the same measures as for SARS? Lancet Infect Dis. 2020; 20: e102- 7.
- Rothan HA, Byrareddy SN. The epidemiology and pathogenesis of coronavirus disease (COVID-19) outbreak. J Autoimmun. 2020; 109: 102433.
- Caruso Chate R, Kaiser Ururahy Nunes Fonseca E, Bastos Duarte Passos R, Borges da Silva Teles G, Shoji H, et al. Presentation of pulmonary infection on CT in COVID-19: Initial experience in Brazil. J Bras Pneumol. 2020; 46: e20200121-e20200121.
- Arentz M, Yim E, Klaff L, et al. Characteristics and Outcomes of 21 Critically Ill Patients with COVID-19 in Washington State. J Emerg Med. 2020; 58: 710-4.
- Onder G, Rezza G, Brusaferro S. Case-Fatality Rate and Characteristics of Patients Dying in Relation to COVID-19 in Italy. JAMA - J Am Med Assoc. 2020; 323: 1775-6.
- Wang L, He W, Yu X, Hu D, Bao M, et al. Coronavirus disease 2019 in elderly patients: Characteristics and prognostic factors based on 4-week follow-up. J Infect. 2020; 80: 639-45.
- Du RH, Liang LR, Yang CQ, Wang W, Cao TZ, et al. Predictors of mortality for patients with COVID-19 pneumonia caused by SARS-CoV-2: A prospective cohort study. Rong-Hui Du, Li-Rong Liang, Cheng-Qing Yang, Wen Wang, Tan-Ze Cao, Ming Li, Guang-Yun Guo, Juan Du, Chun-Lan Zheng, Qi Zhu, Ming Hu, Xu-Yan Li. Eur Respir J. 2020; 56: 2050524.
- Wu Z, McGoogan J. Characteristics of and important lessons from the coronavirus disease 2019(COVID-19) outbreak in China. Jama. 2020; 24: E1-4.
- Hosey MM, Needham DM. Survivorship after COVID-19 ICU stay. Nat Rev Dis Prim. 2020; 6: 60.
- Van Aerde N, Van den Berghe G, Wilmer A, Gosselink R, Hermans G, et al. Intensive care unit acquired muscle weak-ness in COVID-19 patients. Intensive Care Med. 2020; 46: 2083-5.
- Gautam AP, Arena R, Dixit S, Borghi‐Silva A. Pulmonary rehabilitation in COVID‐19 pandemic era: The need for a re-vised approach. Respirology. 2020; 25: 1320-2.
- Severin R, Arena R, Lavie CJ, Bond S, Phillips SA. Respiratory Muscle Performance Screening for Infectious Disease Management Following COVID-19: A Highly Pressurized Situation. Am J Med. 2020; 133: 1025-32.
- Grasselli G, Tonetti T, Protti A, Langer T, Girardis M, et al. Pathophysiology of COVID-19-associated acute respiratory distress syndrome: A multicentre prospective observational study. Lancet Respir Med. 2020; 8: 1201-8.
- Sheehy LM. Considerations for postacute rehabilitation for survivors of COVID-19. J Med Internet Res. 2020; 22.
- Silva RMV da, Sousa AVC de. Fase crônica da COVID-19: Desafios do fisioterapeuta diante das disfunções musculoesqueléticas. Fisioter em Mov. 2020; 33: 2-4.
- Ferraro F, Calafiore D, Dambruoso F, Guidarini S, de Sire A. COVID-19 related fatigue: Which role for rehabilitation in post-COVID-19 patients? A case series. J Med Virol. 2021; 93: 1896-9.
- Tozato C, Ferreira BFC, Dalavina JP, Molinari CV, Alves VLDS. Cardiopulmonary rehabilitation in post-COVID-19 pa-tients: ase series. Rev Bras Ter intensiva. 2021; 33: 167-71.
- Liu K, Zhang W, Yang Y, Zhang J, Li Y, Chen Y. Respiratory rehabilitation in elderly patients with COVID-19: A ran-domized controlled study. Complement Ther Clin Pract. 2020; 39: 101166.
- Silva RN, Goulart CDL, Oliveira MR, Tacao GY, Back GD, et al. Cardiorespiratory and skeletal muscle damage due to COVID-19: making the urgent case for rehabilitation. Expert Rev Respir Med. 2021; 15: 1107-20.
- Klok FA, Boon GJAM, Barco S, Endres M, Miranda Geelhoed JJ, et al. The post-COVID-19 functional status scale: A tool to measure functional status over time after COVID-19. Eur Respir J. 2020; 56.
- Balady GJ, Bricker JT, Chaitman BR, Fletcher GF, Froelicher VF, et al. ACC/AHA 2002 guideline update for exercise testing: summary article: A report of the American college of cardiology/American heart association task force on prac-tice guidelines (committee to update the 1997 exercise testing guidelines) 1 1 The ACC/AHA Task. J Am Coll Cardiol. 2002; 40: 1531-40.
- McConnell AK, Copestake AJ. Maximum static respiratory pressures in healthy elderly men and women: Issues of re-producibility and interpretation. Respiration. 1999; 66: 251-8.
- Luna-Heredia E, Martín-Peña G, Ruiz-Galiana J. Handgrip dynamometry in healthy adults. Clin Nutr. 2005; 24: 250-8.
- Sociedade Brasileira de Cardiologia. III Diretrizes da Sociedade Brasileira de Cardiologia sobre teste ergométrico. Arq Bras Cardiol. 2010; 95: 1- 26.
- Dos Santos TD, Pereira SN, Portela LOC, Cardoso DM, Lago PD, et al. Moderate-to-high intensity inspiratory muscle training improves the effects of combined training on exercise capacity in patients after coronary artery bypass graft surgery: A randomized clinical trial. Int J Cardiol. 2019; 279: 40-6.
- Mohamed Hussein AR, Saad M, Zayan H, Abdelsayed M, Moustafa M, et al. Post-COVID-19 functional status: Relation to age, smoking, hospitalization, and previous comorbidities. Ann Thorac Med. 2021; 16: 260-5.
- Pant P, Joshi A, Basnet B, Shrestha BM, Bista NR, et al. Prevalence of functional limitation in COVID-19 recovered pa-tients using the post COVID- 19 functional status scale. J Nepal Med Assoc. 2021; 59: 7-11.
- Abodonya AM, Abdelbasset WK, Awad EA, Elalfy IE, Salem HA, et al. Inspiratory muscle training for recovered COVID-19 patients after weaning from mechanical ventilation. Medicine (Baltimore). 2021; 100: e25339.
- Silva TCL da, Costa EC, Guerra RO. Resistência aeróbia e força de membros inferiores de idosos praticantes e não-praticantes de ginástica recreativa em um centro de convivência. Rev Bras Geriatr e Gerontol. 2011; 14: 535-42.
- Del Brutto OH, Mera RM, Pérez P, Recalde BY, Costa AF, et al. Handgrip strength before and after SARS-CoV-2 infec-tion in community-dwelling older adults. J Am Geriatr Soc. 2021; 69: 2722-31.
- Tuzun S, Keles A, Okutan D, Yildiran T, Palamar D. Assessment of musculoskeletal pain, fatigue and grip strength in hospitalized patients with COVID-19. Eur J Phys Rehabil Med. 2021; 57: 653-62.