
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 4
Foreign body in rectum- aerosol can
Oscar A Estrada Paz*; Timothy J Young
Division of Pulmonary/Critical Care Medicine, Department of Medicine, UCLA David Geffen School of Medicine, USA.
*Corresponding Author : Oscar A Estrada Paz
Division of Pulmonary/Critical Care Medicine, Department of Medicine, UCLA David Geffen School of Medicine, USA.
Email: oestrada@mednet.ucla.edu,
oscar.estrada23@gmail.com
Received : Sep 27, 2023
Accepted : Oct 27, 2023
Published : Nov 03, 2023
Archived : www.jcimcr.org
Copyright : © Estrada Paz OA (2023).
Keywords: Rectal foreign body; Abdominal pain; Bowel perforation.
Citation: Estrada Paz OA, Young TJ. Foreign body in rectum- aerosol can. J Clin Images Med Case Rep. 2023; 4(11): 2672.
Case presentation
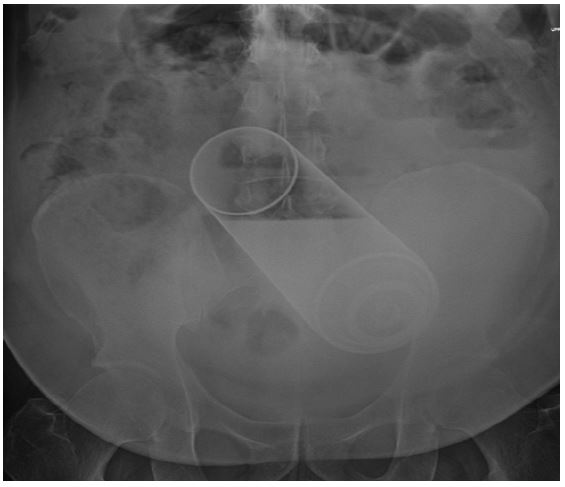
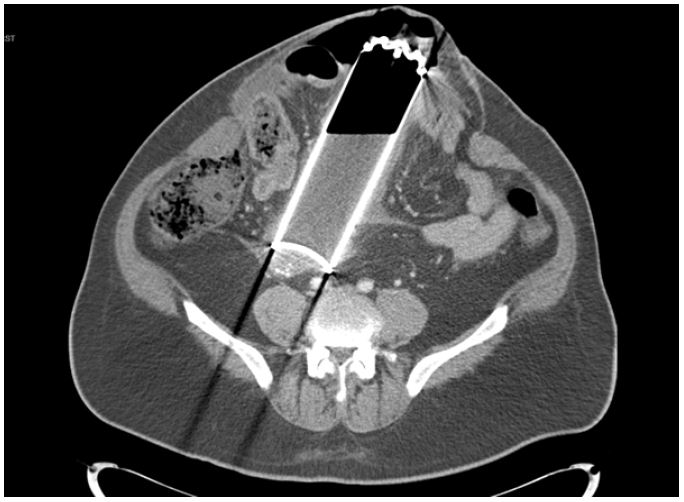
A 53 year-old male with a history of schizophrenia and bipolar disorder presented to the emergency department with worsening abdominal pain. He reported inserting an aerosol can in his anus and was unable to remove the object. The can had been present since midnight the night before. He was concerned that the cap of the can had come loose when he was trying to remove the can from his rectum. On physical exam, his abdomen was distended with a palpable ventral hernia and foreign body. He reported minimal abdominal tenderness with palpation. Abdominal imaging (Figures 1 and 2) demonstrated a large metallic foreign object in the shape of a can in the sigmoid colon with extensive foci of free intraperitoneal air suggestive of bowel perforation. He was immediately taken to the operating room for surgical removal of foreign body. He underwent diagnostic laparoscopy with removal of rectal foreign body, peritoneal lavage, and closure of rectosigmoid perforation. The adhesiolysis portion of the surgical procedure had to be completed using the EndoShears to perform sharp cold adhesiolysis given the aerosol and concern for an intraoperative fire with use of any type of energy or cautery device.
Discussion
Rectal foreign bodies are rare and thus there is no standard approach to diagnosis, technique of removal, and post procedure evaluation [1]. Most patients provide inaccurate histories given that most rectal foreign bodies occur due to self-insertion for sexual gratification [2]. Initial examination of abdomen should be performed to assess for the presence of peritonitis along with a digital rectal exam to assess location and nature of object [3]. Routine radiography can provide important information as to shape and size of object. Some physicians advocate for routine CT imaging for those presenting with rectal foreign bodies for greater than 24 hours [2]. Multiple factors contribute to the approach by the treating physician including size, shape, and composition of the inserted foreign body [3]. Information as to the object inserted can serve as a guide to treatment [2]. Complications such as bowel perforation will also impact decision making as to the selection of treatment approach. The most common anorectal injuries and pathologic changes in self-penetration group include rectal and mucosal ulcers, rectal lacerations and bleeding, but most had an intact rectum. Most patients undergo a transanal surgical procedure for removal with objects that are thick and long presenting the greatest challenge to the operator. These patients may need referral for transabdominal removal [1].
Declarations
Conflict of interest statement: No conflicts of interest.
Funding: There is no source of funding.
Consent: No identifying markers include as part of medical images. No consent required.
References
- Zhang Y, Han Y, Xu H, Chen D, Gao H, et al. A retrospective analysis of transanal surgical management of 291 cases with rectal foreign bodies. Int J Colorectal Dis. 2022; 37: 2167-72.
- Cawich SO, Thomas DA, Mohammed F, Bobb NJ, Williams D, et al. A management algorithm for retained rectal foreign bodies. Am J Mens Health. 2017; 11: 684-92.