
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Diagnostic dilemma- choroidal granuloma as an atypical rare presentation: A case report
Richa Ranjan1*; Sudhir Bhatia2; Bhupesh Singh2; Neha Bharti1; Bhuvan Chanana1; Sudhank Bharti3
1Vitreoretina Consultant, Bharti Eye Foundation and Hospital, New Delhi, India.
2Senior Consultant, Bharti Eye Foundation and Hospital, New Delhi, India.
3Senior Consultant and Director, Bharti Eye Foundation and Hospital, New Delhi, India.
*Corresponding Author : Richa Ranjan
Vitreoretina Consultant Bharti Eye Foundation and Hospital 1/3 East Patel Nagar New Delhi -110008, India.
Tel: 91-8447324405;
Email: richaranjan_2000@yahoo.com
Received : Sep 28, 2023
Accepted : Oct 27, 2023
Published : Nov 03, 2023
Archived : www.jcimcr.org
Copyright : © Ranjan R (2023).
Abstract
Purpose: To report a rare atypical case of ocular toxoplasmosis presenting as choroidal granuloma in a young adult.
Case presentation: A 16-year-old male presented with sudden diminution of vision in the right eye. The visual acuity was 6/12p in the right eye. The anterior segment examination was normal. No relative afferent pupillary defect was present. The fundus examination of the right eye showed grade 1 vitritis, a normal disc with a well circumscribed active choroidal lesion on the posterior pole, inferior to the fovea along with surrounding Subretinal Fluid (SRF) pocket. The Optical Coherence Tomography (OCT) of the right eye showed choroidal elevation with the highest dimension just inferior to the fovea, along with surrounding SRF at the fovea. Fluorescein angiography showed punctate hyperfluorescent leakage points around the lesion.
Intervention: Blood hemogram was normal with a raised erythrocyte sedimentation rate. Serological screening was positive for toxoplasmosis (IgM and IgG antibodies). Human Immunodeficiency Virus (HIV) and tuberculosis (QuantiFERON Gold test) were negative. Oral medications spiramycin 500 mg three times a day for 3 weeks along with folic acid once a day was started after paediatrician consult.
Result: Follow up at 1 week, the visual acuity improved to 6/9 and the choroidal elevation along with the SRF was resolving on the OCT scan. After 3 weeks of treatment the visual acuity improved to 6/6 and the fundus showed complete resolution of the choroidal granuloma along with the surrounding SRF with no residual chorioretinal scar formation.
Conclusions: Our case reports a rare atypical presentation of ocular toxoplasmosis with only one more case available in the literature of ocular toxoplasmosis presenting as a posterior pole choroidal granuloma. Timely intervention lead to complete resolution of the lesion and complete restoration of the visual acuity.
Keywords: Choroidal granuloma; Ocular toxoplasmosis; Atypical presentation.
Abbreviation: SRF: Subretinal Fluid; OCT: Optical Coherence Tomography; TB: Tuberculosis; BCVA: Best Corrected Visual Acuity; IOP: Intraocular Pressure; ESR: Erythrocyte Sedimentation Rate; Mm: Millimeter; HIV: Human Immunodeficiency Virus; HCV: Hepatitis C Virus; Hbsag: Hepatitis B Surface Antigen; VDRL: Veneral Disease Research Laboratory; ACE: Angiotensin Converting Enzyme.
Citation: Ranjan R, Bhatia S, Singh B, Bharti N, Chanana B, et al. Diagnostic dilemma- choroidal granuloma as an atypical rare presentation: A case report. J Clin Images Med Case Rep. 2023; 4(11): 2673.
Introduction
Posterior pole choroidal granuloma can be a presenting feature of various infectious, systemic inflammatory diseases or foreign body [1,2]. Being a country endemic to Tuberculosis (TB), ocular tubercular granuloma is the first diagnosis on seeing a patient with choroidal granuloma. However, a complete general and ocular history with clinical examination along with investigations are important for diagnosis and proper management.
In our report, we present a rare atypical case of ocular toxoplasmosis presenting as a choroidal granuloma in a young patient and discuss the treatment best available for a young adult resulting in complete resolution of the choroidal granuloma and restoration of vision with no residual chorioretinal scarring.
Case presentation
A 16-year-old male patient presented with complains of sudden diminution of vision in the right eye since 5 days. There was no history of any systemic illness or any ocular or head trauma.
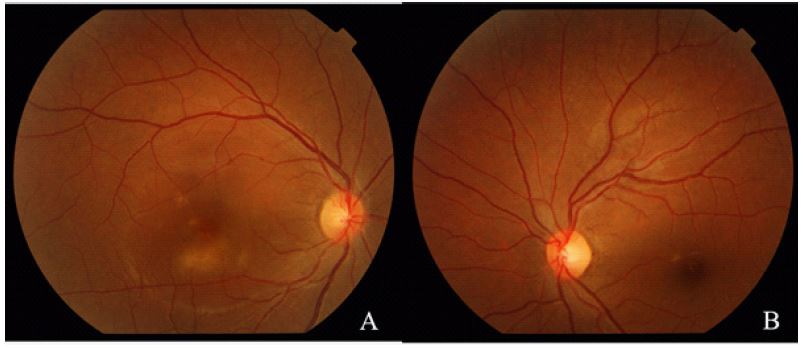
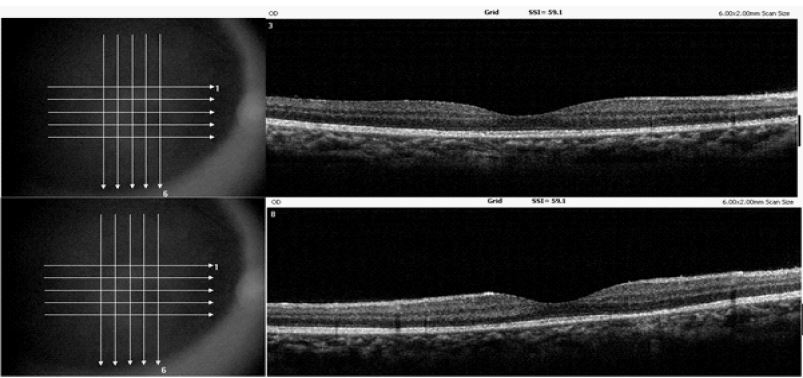
The Best Corrected Visual Acuity (BCVA) was recorded as 6/12p in the right eye and 6/6 in the left eye. The Intraocular Pressure (IOP) recorded with applanation tonometer was 14 mmHg in the right eye and 16 mmHg in the left eye. The anterior segment examination of both the eyes were normal. No relative afferent pupillary defect was present. The fundus examination of the right eye showed grade 1 vitritis, a normal disc with a well circumscribed active choroidal lesion on the posterior pole, inferior to the fovea along with surrounding Subretinal Fluid (SRF) pocket (Figure 1A). The fundus examination of the left eye was normal (Figure 1B). The Optical Coherence Tomography (OCT) of the right eye showed choroidal elevation with the highest dimension just inferior to the fovea, along with surrounding SRF at the fovea (Figure 2). The OCT of the left eye was normal (Figure 3). Fluorescein angiography showed punctate hyperfluorescent leakage points around the lesion (Figure 4). A differential diagnosis of ocular tubercular granuloma, sarcoidosis, choroidal tumor or other infectious uveitic pathology such as in immunocompromised state like syphilis was made.
Blood hemogram was normal with a raised erythrocyte sedimentation rate (ESR-35 millimeter (mm) per hour). Mantoux test showed a 2X2 mm induration after 48 hours. QuantiFERON tuberculosis GOLD test was also negative with a normal High-Resolution Computed Tomography (HRCT) chest scan. Serological screening for Human Immunodeficiency Virus (HIV), Hepatitis C Virus (HCV), Hepatitis B surface antigen (HBsAg) and syphilis (Veneral Disease Research Laboratory-VDRL) were negative. Serological screening for rubella, cytomegalovirus and herpes were negative, however, serological screening for toxoplasma was highly positive (IgM-63.60 AU/mL and IgG-46.40 IU/mL). Serum Angiotensin Converting Enzyme (ACE) for sarcoidosis was within normal limits.
Treatment
Oral medications spiramycin 500 mg three times a day for 3 weeks along with folic acid once a day was started after pediatrician consult. Oral steroids were not started as there was a high clinical suspicion of ocular tubercular granuloma, and so a trial of anti-toxoplasma therapy was initiated for a week and the response was monitored.
Follow up after 1 week, the patient was symptomatically better. The BCVA in the right eye was 6/9. IOP recorded was 14 mm Hg in the right eye. Fundus examination in the right eye showed a healing posterior pole choroidal lesion. The OCT through the lesion showed resolving SRF around the choroidal lesion along with decrease in the vertical dimension of the choroidal elevation (Figure 5).
On seeing a positive response to the treatment, the anti-toxoplasma therapy was continued for another week without starting oral steroids.
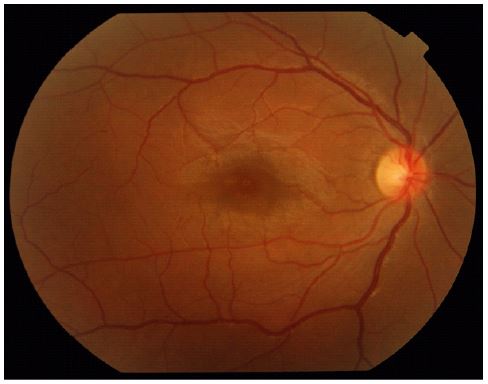
Follow up at 2 weeks, the patient was symptomatically better. The BCVA recorded in the right eye was 6/6. IOP recorded was 14 mmHg. The fundus examination showed complete resolution of the choroidal lesion (Figure 6). The OCT scan showed a normal foveal contour with complete resolution of the choroidal lesion and the surrounding SRF (Figure 7).




The treatment was discontinued. The patient has been under regular follow up. Follow up at 1 year, the patient maintains the BCVA of 6/6 in the right eye with no recurrence of the infection.
Discussion
Ocular toxoplasmosis often presents as focal necrotizing retinitis- a whitish, fluffy lesion with surrounding retinal edema; it is generally associated with vitritis and often granulomatous anterior uveitis, typically termed as headlight in fog appearance [3]. Active lesions can also be classically adjacent to an old inactive chorioretinal scar [3]. The usual age of first presentation of ocular toxoplasmosis is typically in the second decade, and 75% of the cases present between 10 and 35 years of age. Long-term follow-up show the 5-year recurrence rate as 79%, [4] and some patients may have multiple recurrences [5].
Chorioretinitis along with chorioretinal granuloma is a clinical manifestation of a highly inflammatory process that may lead to retinal destruction and scarring. Most common aetiologies include bacterial infection such as Mycobacterium tuberculosis [6] or systemic inflammatory diseases such as sarcoidosis [7] or choroidal tumors or other infectious uveitic pathology such as in immunocompromised state like syphilis. Other bacterial infections such as Treponema pallidum, Bartonella henselae [8], and very rarely Streptococcus pyogenes [9] or fungus such as Candida albicans [10] and Sporothrix schenckii [11] or parasite such as Ascarids especially in children [12] may also produce a granuloma. Other rare cause include foreign body granuloma in intravenous drug users [13].
A small choroidal tumour could mimic a granuloma. Malignant tumour (especially retinoblastoma during childhood) or benign type 2 hamartoma [14] or metastatic tumour (one-third of which are the initial presentation of malignancy-most commonly breast or lung cancer) [15], amelanotic melanoma or lymphoma [16] could look like a granuloma. In our case, however, the presence of posterior uveitis and the hypofluorescence of the lesion in angiography were highly suggestive of a non-neoplastic nature of the lesion.
Our patient presented with the first episode of sudden diminution of vision in the right eye. There was no history of dog or cat exposure, intravenous drug use or risky sexual activity. The patient was non-vegetarian in diet. Being in a country endemic to tuberculosis, the first differential was a choroidal tubercular granuloma. The patient was investigated accordingly for tuberculosis and other differentials also.
Immunosuppression was ruled out due to negative serology reports. The patient was also negative for TB gold quantiFERON test and had a normal chest HRCT scan. All the other investigations were normal, however, the IgG and IgM titre for toxoplasmosis came out to be highly positive.
Choroidal granuloma is an atypical and rare presentation of ocular toxoplasmosis. On review of literature, only one other case of choroidal granuloma secondary to toxoplasmosis has been reported in a Brazilian young female [17]. A provisional diagnosis of ocular toxoplasmosis was made. After a paediatrician consult, the patient was started on a trial of anti-toxoplasma therapy which included tab spiramycin 500 mg three times a day for 3 weeks along with tab folic acid once a day. Being in a country endemic to tuberculosis, ocular tuberculosis was not completely ruled out, despite the investigation being negative for tuberculosis. Oral steroids at this point was not started, considering the patient maybe a case of ocular tubercular granuloma rather than an atypical case of ocular toxoplasmosis. The patient was called after 1 week to see the response of the treatment started and further course of management, whether to change the therapy to anti-tubercular treatment or to start oral steroids. However, follow up at 1 week, the patient was symptomatically better, the vision was improving and the choroidal granuloma was resolving. As the response to the treatment was favourable, the therapy was continued for another 2 weeks without starting oral steroids. Follow up after 2 weeks, the vision had improved to 6/6 and the choroidal granuloma was completely resolved.
Classic therapy of ocular toxoplasmosis consists of 2-4 g of sulfadiazine loading dose given over 24 h, followed by 1 g four times daily and 75-100 mg pyrimethamine loading dose over 24 h followed by 25-50 mg daily. Calcium folinate 2×25 mg is also given to avoid pyremethamine-induced bone marrow depression [17]. Our patient received tab spiramycin after paediatrician consult as it is considered safer in children and pregnant females. Our patient being a young adult, the choice of anti-toxoplasma therapy was spiramycin.
Trimethoprim 80 mg/sulfamethoxazole 400 mg (2 tablets twice a day) or intravitreal clindamycin plus dexamethasone are other alternatives [18,19]. Systemic prednisolone 1 mg/kg body weight is also given to reduce chorioretinal destruction and may be offered in the presence of macula infection or in the case of severe ocular inflammation; however, the risk of complications due to steroids should be weighed, especially in teenagers, as there is no strong evidence of benefit [20,21]. In our patient, steroid therapy was not started due to suspicion of ocular tuberculosis infection owing to the typical choroidal granuloma presentation. Even after 1 week of treatment with no steroid therapy, as the patient showed favourable response, the decision of not starting oral steroid was made, however, the patient was closely followed up. After 3 weeks of anti-toxoplasma therapy the choroidal lesion had completely resolved without any chorioretinal scarring despite no usage of oral steroids, adding to the literature that there is no strong evidence of benefit of oral steroid use in teenagers.
Conclusion
In conclusion, our case reports a rare atypical presentation of ocular toxoplasmosis with only one more case available in the literature of ocular toxoplasmosis presenting as a posterior pole choroidal granuloma [17]. Our case highlights the fact that sometimes common diseases can present with atypical presentation and while treating such patients, sometimes we can go against our clinical knowledge and acumen and follow the path the investigations are leading us to. Timely intervention lead to complete resolution of the lesion and complete restoration of the visual acuity in our patient. Our case also highlights the fact that oral steroids are not necessarily essential in young adults to prevent chorioretinal scar formation after healing of the choroidal granuloma.
Declarations
Consent to participate and publication taken from the patient.
Ethic approval: Not Applicable.
The data and material are available with the corresponding author and can be contacted if needed.
We have no conflict of interest with each other.
We have received no funding for this work from any organization.
We have no financial interest to disclose.
Authors contributions: RR provided clinical care to the patient and prepared the manuscript.
SB provided clinical care to the patient.
BS, NB, BC and SB prepared the manuscript.
The manuscript has been read and approved by all the authors. The requirements for authorship have been met, and each author believes that the manuscript represents honest work.
Acknowledgement: Not applicable.
References
- Panos GD, Papageorgiou E, Kozeis N, Gatziofas Z. Macular hole formation after toxoplasmic retinochoroiditis. BMJ Case Rep. 2013; 2013: bcr2013008915.
- Vasconcelos-Santos DV. Ocular manifestations of systemic disease: Toxoplasmosis. Curr Opin Ophthalmol. 2012; 23: 543-50.
- Park YH, Nam HW. Clinical Features and Treatment of Ocular Toxoplasmosis. Korean J Parasitol. 2013; 51: 393-399.
- Cochereau-Massin I, LeHoang P, Lautier-Frau M, Zerdoun E, Zazoun L, et al. Ocular toxoplasmosis in human immunodeficiency virus-infected patients. Am J Ophthalmol. 1992; 114: 130-135.
- Schuman JS, Weinberg RS, Ferry AP, Guerry RK. Toxoplasmic scleritis. Ophthalmology. 1998; 95: 1399-1403.
- Bowyer JD, Gormley PD, Seth R, Downes RN, Lowe J. Choroidal tuberculosis diagnosed by polymerase chain reaction. A clinicopathologic case report. Ophthalmology. 1999; 106: 290-4.
- Augustin AJ, Boker T, Seewald S, Klassen PM. Solitary retinal granuloma as a presenting sign of sarcoidosis. Ger J Ophthalmol. 1994; 3: 71-2.
- Accorinti M. Ocular bartonellosis. Int J Med Sci. 2009; 6: 131-2.
- Matsuo T, Tamaki M, Oono T. Retinal vasoproliferative granulomatous lesion associated with hand pyoderma caused by Streptococcus pyogenes. Ocul Immunol Inflamm. 2011; 19: 58-61.
- Arroyo JG, Bula DV, Grant CA, Murtha T. Bilateral Candida albicans endophthalmitis associated with an infected deep venous thrombus. Jpn J Ophthalmol. 2004; 48: 30-3.
- Curi AL, Felix S, Azevedo KM, Estrela R, Villar EG, et al. Retinal granuloma caused by Sporothrix schenckii. Am J Ophthalmol. 2003; 136: 205-7.
- Matsuyama K, Ogata N, Takahashi K, Matsumura M, Nishimura T. Case of retinochoroiditis associated with porcine ascarids diagnosed by antibodies in subretinal fluid. Graefes Arch Clin Exp Ophthalmol. 2008; 246: 1065-7.
- Michelson JB, Whitcher JP, Wilson S, Connor GRO. Possible foreign body granuloma of the retina associated with intravenous cocaine addiction. Am J Ophthalmol. 1979; 87: 278-80.
- Good WV, Erodsky MC, Edwards MS, Hoyt WF. Bilateral retinal hamartomas in neurofibromatosis type 2. Br J Ophthalmol. 1991; 75: 190.
- Shields CL, Shields JA, Gross NE, Schwartz GP, Lally SE. Survey of 520 eyes with uveal metastases. Ophthalmology. 1997; 104: 1265-76.
- Ridley ME, McDonald HR, Blumenkranz MS, Zarbin MA, Schachat AP, et al. Retinal manifestations of ocular lymphoma (reticulum cell sarcoma). Ophthalmology. 1992; 99: 1153-61.
- Massa HF, Gatzioufas Z, Mangioris G, Panos GD. Choroidoretinal granuloma in a young female patient. BMJ Case Rep. 2014; 2014: bcr2013200549.
- Baharivand N, Mahdavifard A, Fouladi RF. Intravitreal clindamycin plus dexamethasone versus classic oral therapy in toxoplasmic retinochoroiditis: A prospective randomized clinical trial. Int Ophthalmol. 2013; 33: 39-46.
- Soheilian M, Sadoughi MM, Ghajarnia M, Dehghan MH, Yazdani S, et al. Prospective randomized trial of trimethoprim/sulfamethoxazole versus pyrimethamine and sulfadiazine in the treatment of ocular toxoplasmosis. Ophthalmology. 2005; 112: 1876-82.
- Jasper S, Vedula SS, John SS, Horo S, Sepah YJ, et al. Corticosteroids for ocular toxoplasmosis. Cochrane Database Syst Rev. 2013; 4: CD007417.
- Sahn SA, Lakshminarayan S. Tuberculosis after corticosteroid therapy. Br J Dis Chest. 1976; 70: 195-205.