
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 4
Partial ectopic posterior pituitary
Selma Khouchoua*; Lina Belkouchi; Najlaa Lrhorfi; Siham El Haddad; Nazik Allali; Latifa Chat
Pediatric Radiology Department, Ibn Sina University Hospital Center, Faculty of medicine and Pharmacy of Rabat, Mohammed V University, Rabat, Morocco.
*Corresponding Author : Selma Khouchoua
National Institute of Oncology, UHC Ibn Sina, Mohamed V University, Rabat, Morocco.
Email: selma.khouchoua@gmail.com
Received : Oct 04, 2023
Accepted : Oct 31, 2023
Published : Nov 07, 2023
Archived : www.jcimcr.org
Copyright : © Khouchoua S (2023).
Citation: Khouchoua S, Belkouchi L, Lrhorfi N, El Haddad S, Allali N, et al. Partial ectopic posterior pituitary. J Clin Images Med Case Rep. 2023; 4(11): 2677.
Description
Ectopic posterior pituitary is one of the leading causes of pituitary dwarfism related to a growth hormone deficiency.
It can be either isolated or associated to other abnormalities, the most widely known being the pituitary stalk interruption syndrome [1].
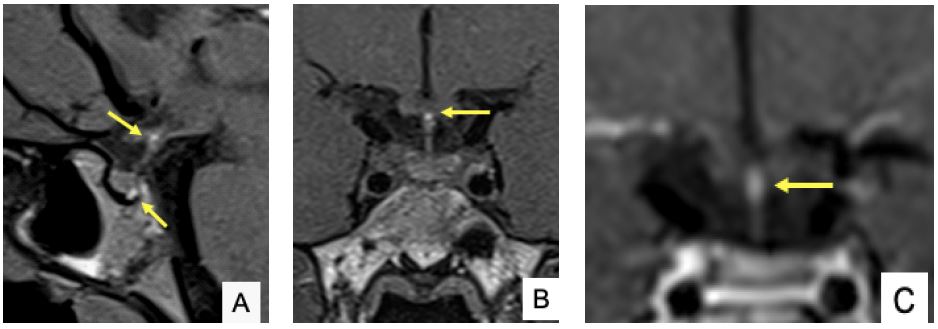
Although it is a rare entity, partial ectopy consists of the coexistence of both an orthotopic and an ectopic posterior pituitary gland [2,3] (Figure 1A). It appears as a T1 hyperintensity or bright spot at the posterior sellae, consistent with the normally expected neurohypophysis [4]. A second midline bright spot located in the infundibulum (Figure 1B), or above the optic chiasm or at the floor of the third ventricle is considered the ectopic posterior pituitary gland. It features high T1 signal intensity with and without fat suppression, making it easy to distinguish from a lipoma or a supra sellar dermoid with lipid content. Contrast enhancement is similar to the normal pituitary parenchyma (Figure 1C).
No pituitary stalk abnormality such as a thinning or absence is typically found. In addition, the anterior pituitary gland shows no signal change or decrease in size, making it easy to make the differential with a pituitary stalk interruption syndrome.
Finally, among the differentials, pituitary hamartomas are typically arising from the tuber cinereum and appear as a T1 hypointense, T2 hyperintense, pedunculated or sessile lesion with no contrast enhancement.
References
- Sridhar S, Raja BR, Priyanka R, Natarajan S, Soundararajan S, et al. Clinico-radiological correlation of pituitary stalk interruption syndrome in children with growth hormone deficiency. Pituitary. 2023; 26: 622-628.
- Ybarra M, Hafiz R, Robinson ME, von Oettingen JE, Bui H, et al. A new imaging entity consistent with partial ectopic posterior pituitary gland: report of six cases. Pediatr Radiol. 2020; 50: 107-115.
- Mészáros F, Vergesslich K, Riedl S, Häusler G, Frisch H. Posterior pituitary ectopy in children with idiopathic growth hormone deficiency. J Pediatr Endocrinol Metab. 2000; 13: 629-35.
- El Sanharawi I, Tzarouchi L, Cardoen L, Martinerie L, Leger J, et al. High-resolution heavily T2-weighted magnetic resonance imaging for evaluation of the pituitary stalk in children with ectopic neurohypophysis. Pediatr Radiol. 2017; 47: 599-605.