
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 4
Overcoming adnexal torsion: Whirlpool sign
Selma Khouchoua*; Lina Belkouchi; Najlaa Lrhorfi; Siham El Haddad; Nazik Allali; Latifa Chat
Pediatric Radiology Department, Ibn Sina University Hospital Center, Faculty of medicine and Pharmacy of Rabat, Mohammed V University, Rabat, Morocco.
*Corresponding Author : Selma Khouchoua
National Institute of Oncology, UHC Ibn Sina, Mohamed
V University, Rabat, Morocco.
Email: selma.khouchoua@gmail.com
Received : Oct 04, 2023
Accepted : Oct 31, 2023
Published : Nov 07, 2023
Archived : www.jcimcr.org
Copyright : © Selma K (2023).
Citation: Marinova L, Georgiev R, Evgeniev N. Clinical observations in three clinical cases with locally advanced chordomas. What is needed for early diagnosis with improved survival?. J Clin Images Med Case Rep. 2020; 1(1): 1005.
Description
Ovarian torsion or adnexal torsion is an acute gynecologic disorder involving complete or partial rotation of the ovarian vascular pedicle. The majority occurs in young women and is mainly associated to an underlying ovarian mass. It remains a challenging diagnosis and imaging plays a pivotal role for timely and accurate diagnosis [1]. In fact, clinical presentation is nonspecific, most patients present with acute abdominal or pelvic pain, either intermittent or persistent with possible nausea and vomiting.
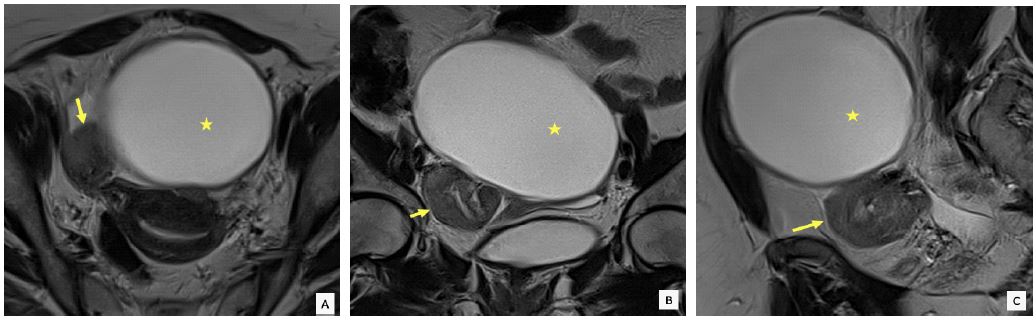
Ultrasound is the first line modality to assess for adnexal torsion, and sonographic findings have been well described. It features an enlarged ovary with or without a mass, peripherally displaced follicles, enlarged and hyperechoic stroma, with abnormal vascular flow doppler. Occasionally the adjacent swirling pedicle can be identified as the whirlpool sign. However, ultrasound examinations are not always conclusive and further MRI examination can be necessary. MRI represents the modality of choice to assess for ovarian torsion. It allows to better analyze the enlarged ovary, to assess for any underlying mass, and to delineate the swirling adnexal vessels [2]. Specific signal characteristics of ovarian masses like cystadenomas, endometriomas or even malignant tumors, allow definitive diagnosis. Multiplanar T2 weighted images, especially in the coronal and sagittal planes, can depict the twisted vascular pedicle as an adjacent small mass in a thickened swirling configuration, next to the main ovarian underlying mass. This appearance is described as the “whirlpool sign”. Visualization of the swirling pedicle is the most pathognomonic and specific feature to make a confident diagnosis. The enlarged ovary usually presents a high T2 signal intensity due to edema. Hemorrhagic alterations can occur featuring high T1 intensity persistent after fat saturation and with low T2 signal intensity. In addition contrast media administration during the MRI examination can show decreased enhancement of the twisted adnexa related to decreased incoming blood supply and is considered more of a prognostic factor. Other MRI features include ascites, uterus deviation towards the torsion, tubal dilatation and possible adnexal fat stranding [3]. Although ultrasound is usually readily available in the emergent setting. MRI appears to be indispensable to make the correct diagnosis. Neglected torsion evolution into abscess formation is exceptional and mortality related to adnexal torsion is very rare. Urgent surgery is the gold standard to prevent ovarian necrosis, unfortunately, salpingo oophorectomy is frequently required.
References
- Tonolini M, Foti PV, Costanzo V, Mammino L, Palmucci S, et al. Cross-sectional imaging of acute gynaecologic disorders: CT and MRI findings with differential diagnosis-part I: corpus luteum and haemorrhagic ovarian cysts, genital causes of haemoperitoneum and adnexal torsion. Insights Imaging. 2019; 10: 119.
- Duigenan S, Oliva E, Lee SI. Ovarian torsion: diagnostic features on CT and MRI with pathologic correlation. AJR Am J Roentgenol. 2012; 198: W122-31.
- Lourenco AP, Swenson D, Tubbs RJ, Lazarus E. Ovarian and tubal torsion: imaging findings on US, CT, and MRI. Emerg Radiol. 2014; 21: 179-87.