
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Right place, wrong pipe: A case of esophageal atresia with atypical tracheal anatomy
Kenneth N John1*; Brenda Satterthwaite2; Elizabeth Renaud3
1Beth Israel Deaconess Medical Center, Department of Anesthesiology, Critical Care, and Chronic Pain 330 Brookline Ave Boston, MA 02215, USA.
2Department of Anesthesiology at Rhode Island Hospital Warren Alpert Medical School of Brown University 593 Eddy Street Providence, RI. 02903, USA.
3Division of Pediatric Surgery Department of Surgery Warren Alpert Medical School of Brown University 593 Eddy Street Providence, RI. 02903, USA.
*Corresponding Author : Kenneth N John
Beth Israel Deaconess Medical Center, Department of Anesthesiology, Critical Care, and Chronic Pain
330 Brookline Ave Boston, MA 02215, USA.
Tel: 518-209-0050;
Email: kjohn1@bidmc.harvard.edu
Received : Oct 05, 2023
Accepted : Nov 01, 2023
Published : Nov 08, 2023
Archived : www.jcimcr.org
Copyright : © John KN (2023).
Abstract
Esophageal Atresia (EA) is an uncommon but serious surgical emergency that typically presents at birth. It can be managed initially with gastrostomy tube placement and a delayed repair, unlike EA with TEF which is typically corrected in the newborn phase. When EA is diagnosed, VACTERL comorbidities must be investigated to assess perioperative risk. This case presents a patient with EA who was found to have an anomalous bronchus intermedius at the carina that was diagnosed using a guidewire and fluoroscopy.
Citation: John KN, Satterthwaite B, Renaud E. Right place, wrong pipe: A case of esophageal atresia with atypical tracheal anatomy. J Clin Images Med Case Rep. 2023; 4(11): 2679.
Introduction
Esophageal Atresia (EA) is an uncommon but serious surgical emergency that typically presents at birth [1]. Diagnosis is confirmed with failure to pass a Nasogastric Tube (NGT) and a chest x-ray showing curling of the NGT in the esophageal pouch [2]. Isolated EA (Gross A, Vogt II) can be managed initially with gastrostomy tube placement and a delayed repair to allow for esophageal growth and primary anastomosis [3]. In this case report, we describe a newborn with radiographic evidence of EA who presented to the operating room for bronchoscopy and gastrostomy tube and ostomy placement. We discuss the patient’s preoperative work up, intraoperative management, and a novel surgical approach that helped evaluate an anomalous airway tract.
Learning objectives
1) Review anesthetic perioperative management of a newborn presenting with EA.
2) Discuss coexisting conditions with EA that elevate risk for perioperative complications.
3) Demonstrate how a surgical and diagnostic technique was able to guide operative and airway management.
Case report
Our patient was an ex-38 week 3-day-old male presenting for a rigid bronchoscopy and esophagoscopy, distal esophagogram, and gastrostomy tube placement for EA without apparent TEF. He was also born with an imperforate anus and was to undergo ostomy creation. After birth, an NGT was unable to be passed and a chest x-ray demonstrated the tube curling in the proximal esophagus. There was no intestinal gas seen on x-ray that led to the presumptive diagnosis of EA without distal TEF. His preoperative evaluation included cardiac, renal, and spine ultrasounds to assess for any additional VACTERL defects. A Transthoracic Echocardiogram (TTE) showed a small Atrial Septal Defect (ASD), and a small to moderate sized patent ductus arteriosus (PDA) with bidirectional flow. The kidneys and spine appeared normal. Preoperative labs included a normal BMP, CBC, capillary blood gas.
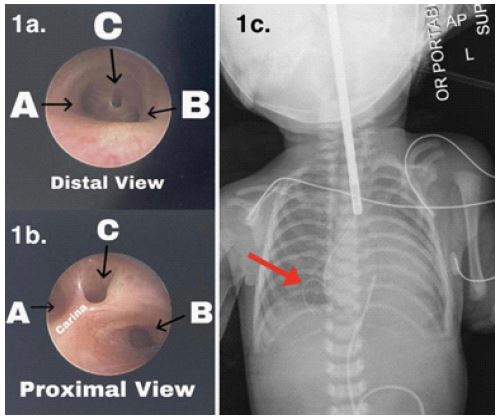
The patient arrived to the OR on 2 lpm of supplemental oxygen. He had an umbilical vein catheter where dextrose- and electrolyte-containing crystalloid and lipid emulsion were infusing. A soft suction catheter was placed in the esophageal stump on continuous suction prior to induction of anesthesia. Standard ASA monitors were applied to the patient. Anesthesia was induced using 80% oxygen/air mixture and sevoflurane 4% in order to maintain spontaneous respirations. For maintenance an IV propofol infusion at 300 mcg/kg/min was used. Hand mask assistance with minimal PEEP (5 mmHg) was implemented to maintain adequate ventilation. During rigid bronchoscopy, the patient remained spontaneously breathing. Once visualizing the trachea, the surgical team noted a defect near the carina (Figure 1a, 1b). They were unable to cannulate the extra orifice with the bronchoscope for further evaluation. A guide wire was inserted through the opening and a chest x-ray revealed the wire extending into the lower lobe of the right lung (Figure 1c). This led us to believe that the extra orifice was the bronchus intermedius originating from the midpoint of the carina. Given the absence of a TEF, muscle relaxation was administered and the patient was intubated. The patient ultimately received a gastrostomy tube and ostomy. The patient remained intubated at the end of the surgery and returned back to the NICU.
Conclusion
Airway management is critical during the intraoperative care of a patient with EA and possible TEF. Typical management involves maintaining spontaneous ventilation to avoid positive pressure due to concern for insufflation of the stomach via a fistula tract. Bronchoscopy can be used to help locate the TEF and guide ETT placement relative to the defect. In this case, when bronchoscopy was performed, we were able to identify an opening in the anterior of the carina but could not determine its tract. We treated it like a TEF and maintained spontaneous ventilation with minimal PEEP. Careful evaluation with a guidewire and fluoroscopy helped to determine the nature of the tract, which was ultimately determined to be an anomalous bronchus.
The original plan for the OR was to perform bronchoscopy and gastrostomy tube and ostomy creation. While this neonate was suspected to have pure EA given his lack of intestinal gas, occasionally a distal TEF can be very small or occluded with secretions that prevent the distal passage of air. Identifying the absence of a TEF was important to guide our patient’s therapeutic approach of feeding and growth to allow for esophageal lengthening [3]. The presence of a TEF would have increased the patient’s susceptibility to pulmonary infections and difficulty with ventilation, prompting surgical correction in the newborn phase [2].
Patients presenting with EA are at risk for coexisting conditions that are commonly referred to as VACTERL (Vertebral anomalies, Anal atresia, Cardiac defects, Tracheo Esophageal fistulas, Renal anomalies, and Limb anomalies) [4]. When a patient is diagnosed with EA, these conditions are screened for in order to best prepare for their anesthetic management. Patients who have EA with TEF, congenital heart disease, poor pulmonary compliance, low birth weight (< 2 kg), and large pericarinal fistulas are at higher risk for perioperative complications [3]. Our patient was 2500 g, had no TEF, had a TTE remarkable for an ASD and PDA, and was easily ventilated with only 5 mmHg of PEEP. These factors, along with a staged surgical approach, made for a relatively lower risk anesthetic.
A novel lesson that can be learned from this case is the usefulness of bronchoscopy, a guidewire, and fluoroscopy to help diagnose the presence and trajectory of a fistula track. Confirming the presence or absence of the TEF is crucial for determining the ultimate surgical repair plan.
Consent: Informed consent was obtained from the legal guardian of our patient.
References
- Gupta Ajit. Tracheoesophgeal Fistula Esophageal Atresia & Anesthetic Management. Indian Jour of Anes. 2002; 46: 353-5.
- Houben CH, Curry JI. Current status of prenatal diagnosis, operative management and outcome of esophageal atresia/tracheoesophageal fistula. Prenatal Diagn. 2008; 28: 667-75.
- Broemling N, Campbell F. Anesthetic Management of Congenital Tracheoesophageal Fistula. Pediatric Anesthesia. 2011; 21: 1092-1099.
- Alp Hayriye. “Esophageal atresia case report”. J Heart and Vasc. 2021; 1.