
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Placenta accreta spectrum in unscarred uterus: A case report in a tertiary facility
Godluck Mlay1; Onesmo Augustino1*; Richard Kiritta1; Godfrey Kaizilege1; Albert Kihunrwa1; Kahibi Bernard1; Kalokosilla Mhando1; Oscar Ottoman2; Mohamed Muyeka2
1Department of Obstetrics and Gynecology, Bugando Medical Centre, Catholic University of Health and Allied Sciences, Tanzania.
2Department of Pathology, Bugando Medical Centre, Catholic University of Health and Allied Sciences, Tanzania.
*Corresponding Author : Onesmo Augustino
Department of Obstetrics and Gynecology, Bugando Medical Centre, Catholic University of Health and Allied Sciences, Tanzania.
Email: onesmolukwaro@gmail.com
Received : Oct 09, 2023
Accepted : Nov 03, 2023
Published : Nov 10, 2023
Archived : www.jcimcr.org
Copyright : © Augustino O (2023).
Abstract
Background: Placenta Accreta Spectrum (PAS) is a broad term that includes placenta accreta, placenta increta, and placenta percreta. The major risk factor is a scarred uterus commonly as a result of prior cesarean delivery, myomectomy, or uterine instrumentation. We report a case of placenta increta in the absence of identifiable risk factors.
Case presentation: A 22-year-old, para 2 living 2, presented with postpartum hemorrhage due to retained placenta post vaginal delivery at a gestational age of 38 weeks and 4 days, manual removal of placenta was attempted general anesthesia without success; necessitating explorative laparotomy where the placenta was found deeply invading into the myometrium. Intractable bleeding necessitated supracervical hysterectomy. Histopathological results later revealed placenta increta.
Conclusion: PAS in an unscarred uterus in the absence of other identifiable risk factors is quite uncommon; however, carries high maternal morbidity and mortality. This case serves as an eye opener on the need to evaluate for radiological features of PAS during antenatal visits even in low-risk group.
Keywords: Placenta accreta spectrum; Placenta increta; Morbid adhere placenta.
Citation: Mlay G, Augustino O, Kiritta R, Kaizilege G, Kihunrwa A, et al. Placenta accreta spectrum in unscarred uterus: A case report in a tertiary facility. J Clin Images Med Case Rep. 2023; 4(11): 2683.
Introduction
Placenta Accreta Spectrum (PAS); is a rare pathology in which trophoblast attach the myometrium (placenta accreta) or invade the myometrium (placenta increta) and occasionally penetrate to or beyond the serosa (placenta percreta). The prevalence ranges from 0.01% to 1.1% [1]. The foremost risk factor is a scarred uterus commonly as a result of prior cesarean delivery, myomectomy, or uterine instrumentation [2-12]. The major morbidity associated with such abnormal placentation primarily arises from the significant blood loss that occurs at the time of delivery. In addition, pregnancies complicated by PAS are thought to be associated with increased incidences of uterine rupture, and invasion of adjacent organs. We report a case of placenta increta in the absence of identifiable risk factors.
Case presentation
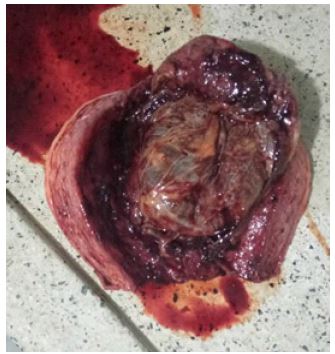
A 22 year old patient, para 2 living 2, she had successful vaginal birth at term. A baby boy of 3.4 kg and APGAR score of 8 and 10 in the first and fifth minutes respectively was delivered and active management of the third stage of labor was initiated. Forty-five minutes following delivery she had retained placental with intractable vaginal bleeding. On examination, she was fully conscious, mildly pale, not jaundiced, and not dyspneic. She had a blood pressure of 116/68 mmHg, pulse rate of 96 beats/minute, respiratory rate of 18 cycles per minute, and body temperature of 36.80 Celsius. On her systemic examination; abdominal examination, she had a boggy, palpable uterus corresponding to 26 weeks GA. On vaginal examination; she had a retained placenta with active vaginal bleeding no vaginal, cervical, or perineal laceration was noted. The diagnosis of postpartum hemorrhage due to retained placental was reached. She was transferred to main theater where under general anesthesia attempt of manual removal of placenta was done but it was unsuccessful, which necessitated emergency explorative laparotomy where the uterus was bulky with placental mass on the fundus left side invading into myometrial tissue, both adnexa appeared macroscopically normal. A supracervical hysterectomy was performed. The uterus was dissected and the placenta was found adhered to it as seen in Figure 1. The sample was kept on 10% neutral buffered formalin and was sent for histopathology evaluation. The histopathological report revealed area with variable size chorionic villi attach and invaginate the smooth muscle stroma conclusion was features of the placenta increta with an area of calcification as seen in Figure 2. Her pre-operative blood workups; she had low hemoglobin of 10.7 g/dl microcytic hypochromic anemia, hematocrit of 34.2%, with platelets of 206 × 103 mm3 which was within normal range. She has blood group A rhesus positive and her bleeding indices were within normal range.

Discussion
Compared to placenta increta and percreta, placenta accreta is far more prevalent [1]. In our case, after histopathological examination, it revealed our patient had placenta increta. The association between prior uterine surgery and the likelihood of placenta previa and PAS is becoming increasingly significant since this progression appears to be directly correlated to damage or lack of the decidua basalis [13]. Risk factors for PAS include prior cesarean delivery, myomectomy, uterine instrumentation and intrauterine scarring, placenta previa, smoking, maternal age over 35 years, grand multiparity and recurrent miscarriage, and history of endometritis [2-12]. In most cases, PAS is a result of a combination of several factors. Contrary to many reports, where PAS has been diagnosed in patients with a scarred uterus [13], our patient had no scarred uterus and no known other risk factor. Cases of PAS in an unscarred uterus have also been reported [14-18].
Previously it was thought PAS was primarily caused by anatomical deficiencies in the decidua (the uterine lining), recent research has suggested that other factors, including the behavior of cytotrophoblasts and angiogenesis (the formation of new blood vessels), may also play a role in the development of PAS. The idea that cytotrophoblasts may control decidual invasion through factors like angiogenesis suggests that these cells may influence the development of PAS by promoting the growth of blood vessels within the uterine tissue. This, in turn, could potentially lead to abnormal placental attachment and invasion of the uterine muscle [19,20]. Moreover, the concept of “hyperinvasiveness” in the context of PAS, refers to the observation that some tissue specimens from patients with PAS exhibit more aggressive and invasive behavior compared to typical placental tissue. This hyperinvasiveness is thought to be related to immunological factors, although the exact mechanisms and triggers are still under investigation [21]. In our case report, we could not establish the risk factor for her perhaps the above theory can support the observation we observed. Furthermore, some genes coding for remodeling and adherence being highly expressed in the context of PAS suggests that specific genes related to tissue remodeling and attachment may play a significant role in the development of this condition. PAS is characterized by abnormal placental attachment and invasion into the uterine wall, and the expression of certain genes can influence these processes [22,23].
Diagnosis of PAS is histologically confirmed; however, due to advancements in imaging it can be predicted before delivery and foresee the anticipated complication. Our patient had obstetric ultrasound taken 3 weeks prior to delivery during the antenatal visit. However, the was no radiological findings reported features suggestive of PAS bearing in mind the sensitivity of ultrasound with doppler color flow is more than (91%) [24]. In our case perhaps we did not focus on the features of PAS possibly because she had no identified risk from the history. This was a missed opportunity for her in our case; however similar cases were reported [14-18].
Conclusion
The placenta accreta spectrum is caries high morbidity and mortality. PAS in an unscarred uterus and in the absence of other identifiable risk factors is quite uncommon, this should encourage us to systematically evaluate patients for PAS during antenatal visits hence, maximize the patient care.
Declarations
Patient’s perspective: The care provided was timely with a full explanation of the diagnosis and prognosis and a follow-up plan explained.
Acknowledgments: We are humbly grateful for the support and encouragement given by the Obstetrics/Gynecology and Central Pathology Laboratory departments at Bugando Medical Centre and Catholic University of Health & Allied Sciences (CUHAS).
Timeline: The patient was admitted on 01/05/2022 and management was initiated immediately. Surgical intervention was done after birth, and the patient was admitted for a total of 4 days. Preparation and completion of the case took 2 months, including follow up and with the case presented to the ethical committee after obtaining consent.
Author’s contribution: GM and OA played equal roles in the preparation of this case report. The other co-authors contributed to the management of the patient and the writing of the case report. All authors read and approved the final manuscript.
Funding: The cost of care offered to this patient was partly covered by the patient and some was waived by the hospital administration. The cost of preparing this manuscript was covered by the authors and the Catholic University of Health and Allied Sciences.
Ethical approval and consent to participate: Written informed consent was obtained from the patient for publication of this case report, and ethical clearance was granted by the Joint Catholic University of Health and Allied Sciences/ Bugando Medical Centre Research and Ethical Review Committee.
Consent for publication: Written informed consent was obtained from the patient for publication of this case and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal. Additionally, consent was sought and granted by the Catholic University of Health and Allied Sciences Directorate of Research and Publication to publish this work. A copy of the clearance document is also available for review by the Editor-in-Chief of this journal.
Competing interests: The authors declare that they have no competing interests.
References
- Jauniaux E, Bunce C, Grønbeck L, Langhoff-Roos J. Prevalence and main outcomes of placenta accreta spectrum: a systematic review and meta-analysis. Am J Obstet Gynecol. 2019; 221: 208-18.
- Silver RM, Landon MB, Rouse DJ, Leveno KJ, Spong CY, et al. Repeat Cesarean Deliveries. Acog. 2006; 107: 1226-32.
- Kohn JR, Shamshirsaz AA, Popek E, Guan X, Belfort MA, et al. Pregnancy after endometrial ablation: A systematic review. BJOG. 2018; 125: 43-53.
- Nageotte MP. Always be vigilant for placenta accreta. Am J Obstet Gynecol. 2014; 211: 87-8.
- Timor-Tritsch IE, Monteagudo A, Cali G, Vintzileos A, Viscarello R, et al. Cesarean scar pregnancy is a precursor of morbidly adherent placenta. Ultrasound Obstet Gynecol. 2014; 44: 346-53.
- Silver RM, Fox KA, Barton JR, Abuhamad AZ, Simhan H, et al. Center of excellence for placenta accreta. Am J Obstet Gynecol. 2015; 212: 561-8.
- Kaser DJ, Melamed A, Bormann CL, Myers DE, Missmer SA, et al. Cryopreserved embryo transfer is an independent risk factor for placenta accreta. Fertil Steril. 2015; 103: 1176-1184.e2.
- Fitzpatrick KE, Sellers S, Spark P, Kurinczuk JJ, Brocklehurst P, et al. Incidence and Risk Factors for Placenta Accreta/Increta/Percreta in the UK: A National Case-Control Study. PLoS One. 2012; 7.
- Hayashi M, Nakai A, Satoh S, Matsuda Y. Adverse obstetric and perinatal outcomes of singleton pregnancies may be related to maternal factors associated with infertility rather than the type of assisted reproductive technology procedure used. Fertil Steril. 2012; 98: 922-8.
- Esh-Broder E, Ariel I, Abas-Bashir N, Bdolah Y, Celnikier DH. Placenta accreta is associated with IVF pregnancies: A retrospective chart review. BJOG. 2011; 118: 1084-9.
- Baldwin HJ, Patterson JA, Nippita TA, Torvaldsen S, Ibiebele I, et al. Antecedents of abnormally invasive placenta in primiparous women: Risk associated with gynecologic procedures. Obstetrics and Gynecology. 2018; 131: 227-33.
- Salmanian B, Fox KA, Arian SE, Erfani H, Clark SL, et al. In vitro fertilization as an independent risk factor for placenta accreta spectrum. Am J Obstet Gynecol. 2020; 223: 568.e1-568.e5.
- Einerson BD, Comstock J, Silver RM, Branch DW, Woodward PJ, et al. Placenta Accreta Spectrum Disorder: Uterine Dehiscence, Not Placental Invasion. Obstetrics and gynecology. 2020; 135: 1104-11.
- Vuong ADB, Nguyen XT, Nguyen PN. Placenta accreta spectrumon an unscarred uterus in the third-trimester pregnancy: two rare cases at Tu Du Hospital in Vietnam. Int J Surg Case Rep. 2022; 99.
- Elkarkri C, Ammouri S, Nah A, Lakhdar A, Zeraidi N, et al. PAMJ-CM-3(69). 2020; 24.
- Enebe JT, Ofor IJ, Okafor II. Placenta percreta causing spontaneous uterine rupture and intrauterine fetal death in an unscared uterus: A case report. Int J Surg Case Rep. 2019; 65: 65-8.
- Malik R, Singh S, Chawla J, Bhardwaj M. Placenta accreta not previa: A rare case report of placenta accreta in an unscarred uterus. Int J Reprod Contracept Obstet Gynecol. 2019; 8: 5050.
- Esmans A, Gerris J, Corthout E, Verdonk P, Declercq S. Placenta percreta causing rupture of an unscarred uterus at the end of the first trimester of pregnancy: Case report. Human Reproduction. 2004; 19: 2401-3.
- Duzyj CM, Buhimschi IA, Laky CA, et al. Extravillous trophoblast invasion in placenta accreta is associated with differential local expression of angiogenic and growth factors: A cross-sectional study. BJOG. 2018; 125: 1441.
- Goh WA, Zalud I. Placenta accreta: Diagnosis, management and the molecular biology of the morbidly adherent placenta. Journal of Maternal-Fetal and Neonatal Medicine. 2016; 29: 1795-800.
- Harris LK, Benagiano M, D’Elios MM, Brosens I, Benagiano G. Placental bed research: II. Functional and immunological investigations of the placental bed. Am J Obstet Gynecol. 2019; 221: 457-69.
- Matsukawa S, Sumigama S, Kotani T, Wang J, Miki R, et al. Possible Association between Cathepsin v and the Development of Placenta Accreta Spectrum Disorders. Gynecol Obstet Invest. 2019; 84: 396-406.
- Shainker SA, Silver RM, Modest AM, Hacker MR, Hecht JL, et al. Placenta accreta spectrum: Biomarker discovery using plasma proteomics. In: American Journal of Obstetrics and Gynecology. Mosby Inc. 2020; 433.e1-433.e14.
- Fratelli N, Fichera A, Prefumo F. An update of diagnostic efficacy of ultrasound and magnetic resonance imaging in the diagnosis of clinically significant placenta accreta spectrum disorders. Current Opinion in Obstetrics and Gynecology. Lippincott Williams and Wilkins. 2022; 34: 287-91.