
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Antisynthetase antibody syndrome complicated by
varicella-zoster virus infection in the
nervous system: A case report
Qinglin Yang*
Department of Neurology, Beijing Tongren Hospital, Capital Medical University, Beijing 100730, China.
*Corresponding Author : Qinglin Yang
Department of Neurology, Beijing Tongren Hospital, Capital Medical University, Beijing 100730, China.
Email: lin8082@sina.com
Received : Oct 09, 2023
Accepted : Nov 03, 2023
Published : Nov 10, 2023
Archived : www.jcimcr.org
Copyright : © Yang Q (2023).
Abstract
Patients with antisynthetase antibody syndrome require long-term oral corticosteroids combined with immunosuppressants, which are prone to immune abnormalities and secondary infections. Varicella-zoster virus is a neurotropic virus that has long been latent in the posterior root of the spinal cord or the trigeminal ganglion. We describe a case of a case of antisynthetase antibody syndrome complicated by varicella-zoster virus infection of the nervous system, confirmed by next-generation sequencing of cerebrospinal fluid pathogens. This case aims to highlight that when a patient with an autoimmune disease and long-term use of immunosuppressants has an invasion of the cranial nerves by the herpes virus, performing imaging and CSF examinations (including etiology) is necessary to clarify the involvement of the central nervous system.
Keywords: Antisynthetase syndrome; Cerebrospinal fluid; Immunosuppressive agents; Varicella-zoster virus.
Citation: Yang Q. Antisynthetase antibody syndrome complicated by varicella-zoster virus infection in the nervous system: A case report. J Clin Images Med Case Rep. 2023; 4(11): 2684.
Introduction
Long-term immunosuppressive therapy increases the risk of opportunistic infection. For example, neurotropic viruses, such as Varicella-Zoster Virus (VZV), which are latent in these patients, become activated and proliferate again, causing infections of the central and peripheral nervous systems. Although imaging and routine cerebrospinal fluid examination can help identify the location and nature of a lesion [1], etiological examination is usually negative [2]. To the best of our knowledge, this is the first report of a case of Antisynthetase Antibody Syndrome (ASS) complicated by VZV infection of the nervous system, confirmed by next-generation sequencing of cerebrospinal fluid pathogens.
Case description
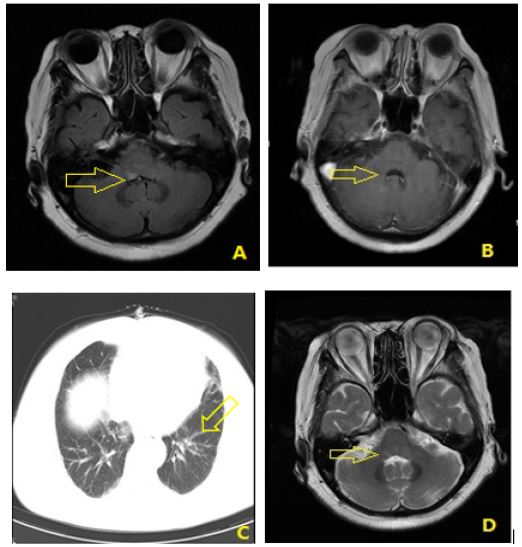
A 59-year-old female patient was admitted to the hospital because of pain in the right glossopharyngeal region for 10 days, which worsened with the inability to close the right eye for 7 days after getting a cold. The stomatology department of a local hospital diagnosed her with glossopharyngeal herpes and prescribed oral acyclovir tablets (the exact dose was unknown). Herpes had developed in the right external auditory canal, along with dizziness, right earache, tinnitus, hearing loss and diplopia in the following day. Moreover, the patient had noticed weakness on the right side of his face, along with closed eyes and drooling and diagnosed with Ramsay Hunt syndrome. Prednisolone (15 mg/d) and vitamin B neurotrophic therapy were administered; however, the symptoms did not considerably improve. Physical examination on admission showed suspected horizontal nystagmus in the left vision. The right eye was weak, right frontal wrinkles were shallow and tympanic cheek was incapable. The tympanic membrane of the right ear was intact with a few white crusts visible on the surface. The patient’s history includes ASS for 5 years, regular oral methotrexate 15 mg/week, and prednisone 15 mg/day. The family history was denied. After admission, she was given antiviral therapy with acyclovir (500 mg Q8H IV) and vitamin B nutrition. In addition, the erythrocyte sedimentation rate was 23 mm/h (normal 0-15 mm/h), antinuclear antibody was 1:320 and anti-Jo-1 antibody was positive. Cerebrospinal fluid pressure (CSF) was 110 mmH2O, white blood cell count was 30 x 106/L (25 mononuclear cells), protein was 231.91 mg/dl, chloride concentration was 140.2 mmol /L, and IgG synthesis rate was 16.20 mg (reference value: 30-0.7/24 hours). CSF cytology showed white blood cells at 1000/0.5 ml, lymphocytes at 90%, immunoglobulin at 77.1 mg/l, and no atypical cells. Serum and CSF were also negative for herpes viruses. Next-generation sequencing of the pathogen from the cerebrospinal fluid detected human herpesvirus-3 (VZV). MRI showed a high-signal lesion in the right posterior medulla oblongatum without obvious enhancement (Figures 1A and 1B). CT showed that interstitial lesions in both lungs with multiple mediastinal lymph nodes visible (Figure 1C).
The patient was discharged after 14 days of intravenous acyclovir treatment and continued to receive oral acyclovir (1 g/day in five divided doses) for another 14 days. One month later, facial paralysis was significantly improved, headaches and dizziness disappeared. The skin of the right external auditory canal was crusted without purulent discharge. CSF protein was 41.18 mg/dl. MRI showed a significant reduction in the abnormal signal intensity in the right posterior medulla oblongata (Figure 1D).
Discussion
ASS is a clinically rare autoimmune disease in the serum characterized by anti-aminoacyl-tRNA synthetase antibodies, mainly anti-Jo-1 positive antibodies. The main symptoms are myositis, interstitial lung disease, Raynaud’s phenomenon, fever, and arthritis [3]. Patients with ASS require long-term oral corticosteroids combined with immunosuppressants, which are prone to immune abnormalities and secondary infections. VZV is a neurotropic virus that has long been latent in the posterior root of the spinal cord or the trigeminal ganglion. Under such conditions, the VZV can be activated and then spread to the nerves. In this case, the lesions involved several areas, including the facial nerve, auditory nerve, glossopharyngeal nerve, and medulla oblongata.
Ramsay Hunt syndrome is the most common cranial nerve damage caused by VZV infection in adults. Multiple cranial nerves can be involved simultaneously, such as the glossopharyngeal nerve and vagus nerve [4]. As imaging and cerebrospinal fluid etiological technology have advanced, additional cases involving the meninges and brain parenchyma have emerged [1,6]. However, cases involving both cranial nerves and brain parenchyma are rare. The patient had autoimmune diseases and had consumed immunosuppressants for a long time. Combined with the clinical manifestations, cranial nerve invasion by VZV was considered. A head MRI after admission showed abnormal signals in the medulla oblongata. Hence, identifying whether the abnormal lesions in the medulla oblongata are directly infected by the virus or demyelinating lesions induced by infection is necessary. Additional routine and biochemical examinations of the CSF confirmed an intracranial infection. Although the cerebrospinal fluid virus antibody and pathogenic bacteria culture were normal, the next-generation sequencing of pathogenic bacteria suggested VZV in the cerebrospinal fluid, implying that virus infection caused medullary abnormalities. The symptoms significantly improved after antiviral treatment. CSF next-generation sequencing can detect the nucleic acid sequence of pathogenic bacteria after amplifying the DNA fragments of pathogenic bacteria in CSF samples, which is more sensitive than traditional methods. This method belongs to the broad screening of pathogens without targeting. Therefore, infection and colonization must be identified along with exogenous nucleic acid contamination [7]. The next-generation sequencing of the patient’s CSF found that the EB virus and Acinetobacter baumannii were present simultaneously. The pathogenic microorganism was excluded owing to its common infection site and good response to antiviral treatment.
This case suggests that when a patient with an autoimmune disease and long-term use of immunosuppressants has an invasion of the cranial nerves by the herpes virus, performing imaging and CSF examinations (including etiology) is necessary to clarify the involvement of the central nervous system. This way, antiviral treatment can be given quickly and properly, and if necessary, prolonged medication can be given.
References
- Edward L, Huseyin T, Mohammed A, et al. Teaching Neuro Images: Classic Ramsay Hunt syndrome and associated MRI findings [J]. Neurology. 2017; 89: e79-80.
- Maria AN, Don G. Neurological Complications of VZV Reactivation [J]. Curr Opin Neurol. 2014; 27: 356-60.
- Li W, LI J, Xie WM, et al. Clinical characteristics of patients with antisynthetase syndrome and interstitial pulmonary disease [J]. Chinese Medical Journal. 2020; 100): 1861-1865.
- Mehmet EK. Multiple cranial nerve injury in Ramsay Hunt Syndrome: A case report [J]. J Pak Med Assoc. 2020; 70:537-538.
- Ji Y, Ma GM, Kang ZL, et al. Ramsay Hunt syndrome with pontine lesion [J], Medicine. 2019; 98: e14260.
- Taesung J, Young CL, Tae GK. Herpes zoster involving the abducens and vagus nerves without typical skin rash: A case report and literature review [J]. Medicine (Baltimore). 2019; 98: e15619.
- Lv J, Guan HZ, Wang DH, et al. Validation of α-herpes viruses in cerebrospinal fluid from patients with intracranial infection by next-generation sequencing[J]. Chin J Neuromed. 2019; 18: 387-391.