
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 4
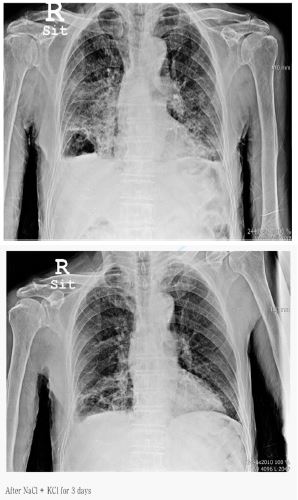
Improvement of graphene induced pulmonary edema by graphene exfoliator NaCl with KCl solution
*Corresponding Author : Chur Chin
Department of Emergency Medicine, New life Hospital Bokhyun-dong, Bukgu, Daegu, Korea.
Email: gemcitabinecisplatin@naver.com
Received : Oct 11, 2023
Accepted : Nov 06, 2023
Published : Nov 13, 2023
Archived : www.jcimcr.org
Copyright : © Chin C (2023).
Citation: Chin C. Improvement of graphene induced pulmonary edema by graphene exfoliator NaCl with KCl solution. J Clin Images Med Case Rep. 2023; 4(11): 2686.
Description
89-year-old man with left basal ganglia internal capsule post limb infarct to our hospital with a history of sputum, fever (37.8oC), dyspnea combined with nasal cannula oxygen therapy, vital signs: blood pressure 120 (systolic) / 60 (diastolic), heart rate 82, respiratory rate 21, O2 saturation 78%, total leukocyte count of 11200/cmm, Lactate Dehydrogenase (LDH) 330 IU/l, alkaline phosphatase 360 u/l, Blood Urea Nitrogen (BUN) 23.7 mg/dl and erythrocyte sedimentation rate (ESR) 50 mm in the first hour using Westergren method, C-reactive protein (CRP) 28.71 mg/dl. The intravenous infusion of a solution consisting of 250 mL normal saline with of potassium chloride (KCl) over 6 h , vitamin C intake with supportive care resulted in recovery of O2 saturation 94%, intramuscular injections of the graphene previously [1-4]. Congestive heart failure (CHF) is the result of insufficient output because of cardiac failure, high resistance in the circulation or fluid overload. Left ventricle (LV) failure is the most common and results in decreased cardiac output and increased pulmonary venous pressure. In the lungs LV failure will lead to dilatation of pulmonary vessels, leakage of fluid into the interstitium and the pleural space and finally into the alveoli resulting in pulmonary edema. Right ventricle (RV) failure is usually the result of long standing LV failure or pulmonary disease and causes increased systemic venous pressure resulting in edema in dependent tissues and abdominal viscera [5]. Abnormal left ventricular structure and function as in, for example, left ventricular hypertrophy or chronic heart failure, is associated with sudden cardiac death and, when the ejection fraction is depressed, with prolongation of the QT interval [6].
References
- Chin C. Comparison of 50 Cases of the Anti-Cancer Effects of NaCl with KCl as a Potent Graphene Exfoliator, Prehydrated Patients to NaCl-Only Prehydrated Patients on the Terminal Stage Cancer Patients. Case Reports in Clinical Medicine. 2023; 12: 425-431. DOI:10.4236/crcm.2023.1210057
- Chin C. Changes in electrocardiogram after intramuscular injection of graphene using salt- intercalation exfoliation, J ClinExp Cardiol. 2023; 14(5): 1-15.
- Chin C. Cell entry inhibitor with sulfonated colloid gold as new potent broad spectrum virucides. J Infect Dis Ther. 2021; 9(4): 1-4.
- Chin C. The Anti-Inflammatory Effects of NaCl with KCl as a Potent Graphene Exfoliator in a Patient with Guillaine-Barré Syndrome and Facial Nerve Palsy, Case Reports in Clinical Medicine. 2023; 12: 447-451. https://www.scirp.org/journal/crcm
- AuVW, JohnsDN, Slavotinek JP. Pulmonary hypertension secondary to leftsided heart disease: A cause for ventilation-perfusion mismatch mimicking pulmanaryembolism.British Journal of Radiology 2001; 74(877): 86-88.
- P P Davey, C Barlow, G hart. Prolongation of the QT interval in heart failure occurs at low but not at high heart rates. ClinSci (Lond). 2000; 98(5): 603-610.