
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Repeated mechanical thrombectomy in recurrent ischemic stroke due to large vessel occlusion: A case report and literature review
Sergio Soeren Rossi1; Gianmarco Iaccarino1; Michele Alessiani1; Adriano Bonura1; Maria Cristina Bravi2;
Domenica Crupi2;
Chiara De Fino2; Marilena Mangiardi2; Francesca Romana Pezzella2; Elisa Testani2;
Sebastiano Fabiano3; Gianluca De Rubeis3; Sabrina Anticoli2*
1Department of Medicine, Neurology, Neurophysiology & Neurobiology Unit, Campus Bio-Medico University Hospital, Rome, Italy.
2Head, Neck and Neuroscience Department, Stroke Unit, San Camillo-Forlanini Hospital, Rome, Italy.
3Diagnostic and Interventional Neuroradiology Department, San Camillo-Forlanini Hospital, Rome, Italy.
*Corresponding Author : Sabrina Anticoli
Head, Neck and Neuroscience Department, Stroke Unit, San Camillo-Forlanini Hospital, Rome, Italy.
Email: sabrina.anticoli@gmail.com
Received : Oct 16, 2023
Accepted : Nov 08, 2023
Published : Nov 15, 2023
Archived : www.jcimcr.org
Copyright : © Anticoli S (2023).
Abstract
Introduction: Recurrent acute ischemic stroke due to large vessel occlusion is a rare condition that primarily affects patients with cardioembolic risk factors. This condition is more frequent in patients who lack sufficient anticoagulation therapy.
Case presentation: We present a case of a 77-year-old woman with paroxysmal atrial fibrillation experienced an acute ischemic stroke due to occlusion of the M2 segment of the left middle cerebral artery. She underwent successful mechanical thrombectomy, leading to revascularization. However, two hours after the procedure, she developed acute left hemiplegia caused by occlusion of the proximal right middle cerebral artery. Another successful mechanical thrombectomy was performed. After a hospital stay of 7 days, the patient was discharged, exhibiting complete regression of the neurological symptoms.
Conclusion: Although literature on this subject is limited, available data indicate that repeated mechanical thrombectomy is an effective and safe procedure.
Keywords: Stroke; Recurrent ischemic stroke; Repeated mechanical thrombectomy; Large vessel occlusion; Cardioembolism; Anticoagulants.
Citation: Rossi SS, Iaccarino G, Alessiani M, Bonura A, Anticoli S, et al. Repeated mechanical thrombectomy in recurrent ischemic stroke due to large vessel occlusion: A case report and literature review. J Clin Images Med Case Rep. 2023; 4(11): 2689.
Introduction
Stroke is the second most common cause of mortality and disability worldwide [1]. Following a first Acute Ischemic Stroke (AIS), the risk of recurrence within 5 years is 24% for females and 42% for males [2]. The highest risk of recurrence is within the first 2 weeks after the initial stroke [2]. Approximately 30% of ischemic strokes are caused by large vessel occlusion (LVO) [3-7], that refers to the obstruction of major cerebral arteries (the intracranial Internal Carotid Artery (ICA), the first and second segments (M1,M2) of the Middle Cerebral Artery (MCA), the first segment (A1) of the Anterior Cerebral Artery (ACA), the Basilar Artery (BA), and the first segment of the Posterior Cerebral Artery (PCA). Stroke due to LVO is associated with higher rates of disability and mortality within 3-6 months compared to non-LVO AIS [7].
Intrarterial treatment with mechanical thrombectomy is effective for reducing disability due to acute ischemic stroke caused by large vessel occlusion and it is the standard treatment (in addition to endovenous thrombolysis) for AIS if performed within 6 hours since symptom onset [8-10]. According to results from the trials DAWN and DEFUSE-3, MT is an effective and safe procedure when it is used from 6 to 24 h from symptoms onset in patients with specific perfusion imaging and medical history features [24,25]. Recurrence of stroke resulting from large vessel occlusion can occur during the early period after mechanical thrombectomy in up to 9% of patients [3]. Despite the absence of clear guidelines in this regard, it is reasonable to subject these patients to a second mechanical thrombectomy. In this paper, along with a brief literature review, we present the emblematic case of a patient who, after the recurrence of ischemic stroke due to bilateral occlusion of the middle cerebral arteries, underwent a repeated mechanical thrombectomy procedure just a few hours after the first one.
Case description
A 77 years old woman presented to the emergency department with symptoms of right hemiparesis and speech disturbance that had started 2 hours before. Her medical history was notable for hypertension, atrial sinus node disease treated with PMK implantation 20 years before, and paroxysmal atrial fibrillation for which she took a daily dose of 15 mg Rivaroxaban. She was taking a reduced dose of Rivaroxaban due to a slight decrease in glomerular filtration rate.
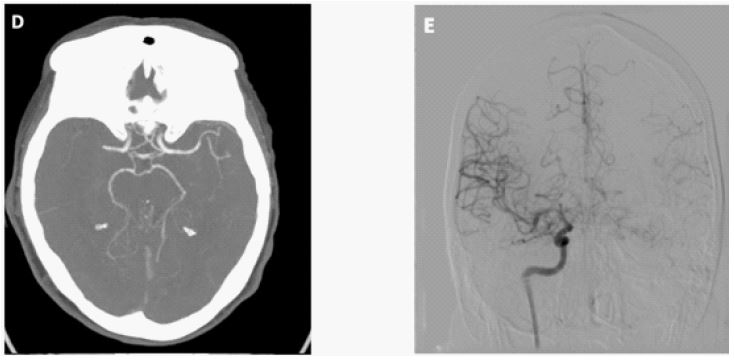
Upon neurological examination, the patient exhibited moderate aphasia, flattening of the right nasolabial fold, mild weakness in the right upper and lower limbs, and mild sensory loss on the right hemisoma (NIHSS 11). A Computed Tomography Angiography (CTA) revealed an occlusion of the M2 segment of the left middle cerebral artery (MCA) (Figure 1A and B). Due to recent intake of Rivaroxaban, the patient was not eligible for intravenous thrombolysis. Within 3 hours of symptom onset, endovascular thrombectomy was performed, resulting in excellent recanalization (a score of 2c on the modified thrombolysis in cerebral infarction scale) (Figure 1C). No parenchymal hemorrhage was observed on the post-procedural head CT scan. The patient experienced a significant improvement in her neurological symptoms immediately after the procedure, with only slight right hemiparesis and no speech disturbance (NIHSS 3). However, two hours after the thrombectomy, she developed new neurological symptoms. At neurological examination she presented complete lower facial palsy on the left side, left hemiplegia in the upper and lower limbs, and moderate dysarthria (NIHSS 12). Another CTA was performed, which revealed an acute occlusion of the M1 segment of the right MCA (Figure 2D).
Within one hour since the appearance of the new symptoms, a repeated mechanical thrombectomy was performed, resulting in successful revascularization (mTICI3) (Figure 2E). The post-procedural CT scan showed no intracerebral hemorrhage.
The patient was then admitted to the stroke unit. The blood tests that were run during her hospital stay revealed a slight dyslipidemia (LDL 173 mg/dl) and a slight decrease in glomerular filtration rate (44 ml/min). Twenty-four hours after the second procedure, another CT scan was performed, which showed an ischemic lesion in the head of the right caudate and lentiform nuclei, as well as in the left lenticular-insular center.
The transthoracic echocardiogram revealed a slight reduction in ejection fraction (47%), moderate left atrial dilatation, and no evidence of intrachamber thrombi or hypokinetic areas. Additionally, a transesophageal echocardiogram was performed, which showed an intact atrial septum, a thrombus-free left atrial appendage, and no signs of valvular vegetations. Throughout her hospitalization, the patient experienced a complete recovery from her symptoms (NIHSS 0) and was discharged home after 7 days. Due to the pacemaker device, magnetic resonance imaging was not feasible, but a CT scan performed 5 days later confirmed the stability of the ischemic lesions. The anticoagulant therapy was changed to apixaban 5 mg twice daily.
Literature review
Recurrence of ischemic stroke due to large vessel occlusion is a potentially life-threatening event that necessitates appropriate treatment, with atrial fibrillation-induced cardioembolism being the most common cause, followed by large artery atherosclerosis [2-6]. In patients with cardioembolic ischemic stroke, the risk of recurrence ranges from 1-22%, with a mean time of 12 days between the two events [6]. This condition is more frequent in patients who lack sufficient anticoagulation therapy [5]. The higher rate of recurrence observed in patients with cardioembolic stroke may be explained by the fact that patients with intracranial or extracranial atherosclerosis often undergo stenting or endarterectomy [20]. Other causes of reocclusion include periprocedural vessel dissection and stent thrombosis [2].

Limited literature is available regarding repeated mechanical thrombectomy (rMT) in cases of short-term recurrent LVO stroke, primarily consisting of retrospective cohort studies. The available data suggest that the percentage of patients undergoing rMT ranges from 0.4% to 1.8%. However, it is reasonable to assume that these figures do not accurately reflect reality because (1) patients experiencing repeated LVO may seek care at different hospitals, (2) clinical deterioration may go unnoticed in severely disabled patients, or (3) only patients demonstrating significant clinical improvement after the initial mechanical thrombectomy are considered suitable candidates for a second procedure [14].
Predictors of unexpected early reocclusion (within 48 hours of the first mechanical thrombectomy) include a high platelet count (>220 g/L) upon admission, residual thrombus or stenosis missed after the initial thrombectomy, occlusion at the M2 site as the initial occlusion site, stroke of undetermined source, a higher number of passes during thrombectomy, transient reocclusion during the procedure [13-18]. Intraoperative reocclusion corresponds to an unstable occlusion site [18]. Additionally, a negative association has been found between pretreatment statin therapy and vessel reocclusion [18].
In a review conducted by Styczen and colleagues [4], it was observed that 50% of the cohort (29 out of 58 patients) experienced reocclusion of the same vessel. Similar findings were presented in the review by Ghada et al. [2], where occlusion of the same artery was reported in 59% of the reviewed cases. It might be presumed that arterioembolism is more likely to cause repeated occlusions of the same artery, while cardioembolism may result in strokes affecting different arterial territories. However, an interesting finding by Ghada and colleagues was that cardioembolism was the most common mechanism leading to occlusion of the pretreated artery [2]. Several hypotheses have been proposed, including aortic arch anatomy, hemodynamics, and laminar flow patterns [2]. Previous studies have also indicated that mechanical thrombectomy induces changes in the vessel wall, such as endothelial denudation, disruption of the internal elastic lamina, and edema in the intimal and medial layers [15-17]. Endothelial injury has been observed following the use of both stent retrievers and aspiration techniques [16-21] with higher frequency among patients treated with mechanical thrombectomy after receiving recombinant tissue Plasminogen Activator (r-tPA) due to the plasminogen activator’s potential to increase metalloproteinase activity [15]. Although there is no definitive evidence to support the notion that the damage caused by mechanical thrombectomy leads to recurrent stroke [20], these findings, coupled with vessel alterations resulting from oxidative stress and inflammation following brain ischemia, provide support for the potential benefits of vasculoprotective therapies [15]. Furthermore, given that both intracranial and extracranial vessel lesions are detected in patients with recurrent strokes, a thorough evaluation of the final angiographic runs should be conducted before removing the catheter to identify flow-modifying lesions that may have pre-existing or iatrogenic origins [22].
Repeated mechanical thrombectomy is a technically feasible and safe procedure [14]. Reported complications include subarachnoid hemorrhage [20], intracerebral hemorrhage [2,14,23], and aspiration pneumonia during the post-operative period [14,20].
A noteworthy finding highlighted by Styczen et al. [4], who analyzed a group of 30 patients who underwent two thrombectomy procedures within 30 days due to recurrent LVO, was that patients with recurrent LVO in the contralateral hemisphere or occlusions in both the anterior and posterior territories exhibited reduced functional independence (mRS 0-2: 30% vs. 56%, p=0.066) and higher mortality rates (mRS 6: 40% vs. 6%, p=0.001) compared to patients with LVO recurrence in the same territory [4]. In fact, Elfil et al., in their meta-analysis, emphasized a correlation between a favorable outcome and the laterality of the second stroke, with a significantly lower percentage of favorable outcomes observed for second mechanical thrombectomy in the contralateral hemisphere compared to the same hemisphere [3]. Consistent literature data indicate that patients with ipsilateral recurrence experience a significantly higher rate of good clinical outcomes compared to patients with contralateral recurrence [3,19].
Apparently, there is no significant association, in both mechanical thrombectomies, between favorable outcomes and age, ASPECT score, TICI score, duration between the first and second stroke, or stroke etiology [3]. Most patients demonstrate considerable improvement in their baseline NIHSS score after the first mechanical thrombectomy [4]. In a study by Elfil et al., the second mechanical thrombectomy achieved successful recanalization in 86.6% of cases, compared to 92.7% after the first mechanical thrombectomy. Regarding the 24-hour NIHSS score, the second mechanical thrombectomy resulted in a mean improvement of 5.97 points, compared to 8.91 points after the initial procedure. Moreover, patients undergoing repeated mechanical thrombectomy exhibit favorable outcomes in terms of mortality and long-term disability, as evaluated by mRS scores of 0-3 at 90 days [3]. However, it should be noted that a selection bias may be present as patients undergoing repeated mechanical thrombectomy may have been chosen based on favorable clinical profiles.
Discussion
In this case report, the recurrence of Large Vessel Occlusion (LVO) was attributed to a cardioembolic mechanism. The inadequacy of anticoagulant therapy was likely due to the insufficient dosage of Rivaroxaban. The selection of therapy should be individualized based on the patient’s specific needs and comorbidities, with preference given to medications that can be administered at a full dose. We opted for Apixaban as the new anticoagulant therapy, as the patient did not have any contraindications to receiving the full dose. This case report emphasizes that patients who undergo double short-term mechanical thrombectomy for recurrent Acute Ischemic Stroke (AIS) with LVO can achieve favorable clinical outcomes. It also highlights that repeated mechanical thrombectomy should be considered as a therapeutic option, as it can yield similar results to patients undergoing a single thrombectomy. Currently, European guidelines do not provide specific recommendations for the treatment of patients with acute ischemic stroke resulting from recurrent large vessel occlusion. Further studies and Randomized Controlled Trials (RCTs) are necessary to evaluate the true effectiveness and safety of repeated mechanical thrombectomy, providing more evidence on the expected clinical outcomes in terms of short- and long-term disability and identifying factors that may influence these outcomes. Although existing literature reports on cases have shown promising data, additional research is needed.
Conclusion
In conclusion, the occurrence of a first mechanical thrombectomy should not deter consideration of a repeated procedure, as patients may achieve similar favorable outcomes compared to the current literature pertaining to single thrombectomy.
References
- Matthew J Kercher, Dinesh Ramanathan, Brian C Dahlin, Alan H Yee, Jared W Clouse, et al. Mechanical Thrombectomy for Sequential Bilateral Middle Cerebral Artery Occlusions in a Patient With Recurrent Cryptogenic Strokes: A Case Report, Neurohospitalist. 2021; 11: 54-58.
- Ghada A Mohamed, Hassan Aboul Nour, Raul G Nogueira, Mahmoud H Mohammaden, Diogo C Haussen, et al. Repeated Mechanical Endovascular Thrombectomy for Recurrent Large Vessel Occlusion, Stroke. 2021; 52: 1967-1973.
- Mohamed Elfil, Eshak I Bahbah, Ahmed Bayoumi, Mohammad Aladawi, Mohamed Eldokmak, et al. Repeated mechanical thrombectomy for recurrent large vessel occlusion: A systema9c review and meta-analysis, IntervenEonal Neuroradiology. 2022; 15910199221134307.
- Hanna styczen, chrisEan Maegerlein, leonard ll Yeo, chrisEn clajus, andreas Kastrup, et al. Repeated mechanical thrombectomy in short-term large vessel occlusion recurrence: Mul9center study and systema9c review of the literature, J. Neurointerv Surg. 2020; 12: 1186-1193.
- Ralph Weber, Paul Stracke, René Chapot. Time Point, E9oglogy, and Short-Term Outcome of Repeated Mechanical Thrombectomy Due to Recurrent Large Vessel Occlusion, FronEers in Neurology. 2019; 10: 204.
- Bouslama M, Haussen DC, Rebello LC, Grossberg JA, Frankel MR, et al. Repeated Mechanical Thrombectomy in Recurrent Large Vessel Occlusion Acute Ischemic Stroke, IntervenEonal Neurology. 2017; 6: 1-7.
- Malhotra K, Gornbein J, Saver JL. Ischemic strokes due to large-vessel occlusions contribute disproportionately to stroke-related dependence and death: A review. Front Neurol. 2017.
- Rennert RC, Wali AR, Steinberg JA, Santiago-Dieppa DR, Olson SE, et al. Epidemiology, Natural History, and Clinical Presentation of Large Vessel Ischemic Stroke. Neurosurgery. 2019; 85: S4-S8.
- Campbell BC, Donnan GA, Lees KR, et al. Endovascular stent thrombectomy: The new standard of care for large vessel ischaemic stroke. Lancet Neurol. 2015; 14: 846.
- Goyal M, Menon BK, van Zwam WH, et al. Endovascular thrombectomy after large-vessel ischaemic stroke: A meta-analysis of individual patient data from five randomised trials. Lancet. 2016; 387: 1723.
- Albers GW, Marks MP, Kemp S, et al. DEFUSE 3 Investigators. Thrombectomy for stroke at 6 to 16 hours with selection by perfusion imaging. N Engl J Med. 2018; 378: 708-18.
- Nogueira RG, Jadhav AP, Haussen DC, et al. DAWN Trial Investigators. Thrombectomy 6 to 24 hours after stroke with a mismatch between deficit and infarct. N Engl J Med. 2018; 378: 11-21.
- Mosimann PJ, Kaesmacher J, Gautschi D, Bellwald S, Panos L, et al. Predictors of Unexpected Early Reocclusion After Successful Mechanical Thrombectomy in Acute Ischemic Stroke Patients. Stroke. 2018; 49: 2643-2651.
- Pirson FAV, van Oostenbrugge RJ, van Zwam WH, Remmers MJM, Dippel DWJ, et al. Repeated Endovascular Thrombectomy in Patients with Acute Ischemic Stroke: Results from a Nationwide Multicenter Database. Stroke. 2020; 51: 526-532.
- Renú A, Laredo C, Lopez-Rueda A, Llull L, Tudela R, et al. Vessel Wall Enhancement and Blood-Cerebrospinal Fluid Barrier Disruption After Mechanical Thrombectomy in Acute Ischemic Stroke. Stroke. 2017; 48: 651-657.
- Teng D, Pannell JS, Rennert RC, Li J, Li YS, et al. Endothelial trauma from mechanical thrombectomy in acute stroke: In vitro live-cell platform with animal validation. Stroke. 2015; 46: 1099-106.
- Peschillo S, Diana F, Berge J, Missori P. A comparison of acute vascular damage caused by ADAPT versus a stent retriever device after thrombectomy in acute ischemic stroke: A histological and ultrastructural study in an animal model. J Neurointerv Surg. 2017; 9: 743-749.
- Marto JP, Strambo D, Hajdu SD, Eskandari A, Nannoni S, et al. Twenty-Four-Hour Reocclusion After Successful Mechanical Thrombectomy: Associated Factors and Long-Term Prognosis. Stroke. 2019; 50: 2960-2963.
- Lee HJ, Kwak HS, Chung GH, Park JS. Repeated Endovascular Thrombectomy in Patients with Acute Ischemic Stroke in a Single Center. J Stroke Cerebrovasc Dis. 2021; 30: 105457.
- Bhogal P, AlMatter M, Hellstern V, Pérez MA, Ganslandt O, et al. Mechanical thrombectomy for recurrent large vessel occlusion. J Clin Neurosci. 2019; 66: 107-112.
- Gory B, Bresson D, Kessler I, Perrin ML, Guillaudeau A, et al. Histopathologic evaluation of arterial wall response to 5 neurovascular mechanical thrombectomy devices in a swine model. AJNRAm J Neuroradiol. 2013; 34: 2192-8.
- Ikenberg B, Rösler J, Seifert CL, Wunderlich S, Kaesmacher J, et al. Etiology of recurrent large vessel occlusions treated with repeated thrombectomy. Interv Neuroradiol. 2020; 26: 195-204.
- Klepanec A, Harsany J, Haring J, Mako M, Hoferica M, et al. Endovascular treatment of acute ischemic stroke in patients with recurrent intracranial large vessel occlusion. Interv Neuroradiol. 2020; 26: 376-382.
- Nogueira RG, Jadhav AP, Haussen DC, Bonafe A, Budzik RF, et al. DAWN Trial Investigators. Thrombectomy 6 to 24 Hours after Stroke with a Mismatch between Deficit and Infarct. N Engl J Med. 2018; 378: 11-21.
- Albers GW, Marks MP, Kemp S, Christensen S, Tsai JP, et al. DEFUSE 3 Investigators. Thrombectomy for Stroke at 6 to 16 Hours with Selection by Perfusion Imaging. N Engl J Med. 2018; 378: 708-718.