
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Infra-renal aortic intra-mural hydatid cyst: An extremely rare localization
Mohammad Ali Nahas1; Hammoud Hamed2; Ashraf Mohammed3*; M-Fadi Alkurdi4; Zaher Al Nahhas5;
Ali Shaddoud6; Mohammed Jomaa7; Omar Tasabehgi8
1Head of Vascular and Endovascular Surgery Department, Al-Assad University Hospital, Faculty of Medicine, Damascus University, Syria.
2Professor of General and Laparoscopic Surgery, Faculty of Medicine, University of Damascus, Syria.
3Vascular Surgery Specialist, Al-Assad University Hospital, Damascus, Syria.
4Department of Surgery, Faculty of Medicine, Damascus, Syria.
5Radiology Resident, Damascus Hospital, Damascus, Syria.
6Vascular Surgery Resident, Damascus University Hospitals, Damascus, Syria.
7General and Laparoscopic Surgery Resident, Faculty of Medicine, Damascus University.
8Medical Student, Al-Sham Private University, Damascus, Syria.
*Corresponding Author : Ashraf Mohammed
Vascular Surgery Specialist, Al-Assad University Hospital, Damascus, Syria.
Tel: +96 3937590017;
Email: drashrfmohammed90@gmail.com
Received : Oct 10, 2023
Accepted : Nov 08, 2023
Published : Nov 15, 2023
Archived : www.jcimcr.org
Copyright : © Mohammed A (2023).
Abstract
Introduction: Hydatid cysts are parasitic infections caused by ecchinococcus granulosus. They usually infect the liver and the lungs in 90% of cases, while the abdominal aortic localization is extremely rare. Aortic infection might lead to serious complications such as ischemia, pseudo-aneurysm formation and anaphylaxis.
Case presentation: 55 years old male patient who was followed up because of lower limb intermittent claudication and lower back pain presented to the emergency department with refractory vomiting complaint. Small bowel obstruction was diagnosed. Laparotomy evidenced adherences between the third portion of the duodenum and the infra-renal aorta. Gastro-jejunal anastomosis was performed. Two weeks later, the aorta was resected and replaced by aorto-bi-iliac 8/16 mm bifurcated collagen impregnated dacron graft.
Results: Total relief of abdominal and vascular symptoms was obtained . Normal follow up.
Conclusion: Hydatid cyst is very frequent in poor and rural areas. Liver and Lungs represent the most organs infected. The vascular localizations are very rare, and they must be taken in consideration in case of para-aortic cystic lesions. Imaging modalities such as multi-slice computed tomography with 3D reconstruction and MRI can provide more detailed assessment of the relationship between the cyst and adjacent structures. Digital Subtraction Arteriography (D.S.A.) remains the gold standard to study the connection between cystic cavity and aortic lumen. Serological tests, including Enzyme-Linked Immunosorbent Assays (ELISA), can help the diagnostic process by confirming the infection by Echinococcosis granulosus. Surgical resection and vascular axis reconstruction is the only treatment option which can be preceded, in some case, by endovascular stent graft bridging.
Keywords: Infra-renal abdominal aorta; Hydatid cyst; Echinococcal disease.
Citation: Ali Nahas M, Hamed H, Mohammed A, Alkurdi MF, Al Nahhas Z, et al. Infra-renal aortic intra-mural hydatid cyst: An extremely rare localization. J Clin Images Med Case Rep. 2023; 4(11): 2690.
Introduction
Hydatid cyst is a parasitic infection caused by the tapeworm of the genus Echinococcus. Among the known species of the echinococcus, the most common is the echinococcus granulosus, which causes the cystic form of this zoonotic infection “hydatid cysts” [1]. Humans are incidental intermediate hosts of this parasite who might be infected by exposure to food and water contaminated by the feces of an infected definitive host especially in rural areas or poor hygiene [2].
Hydatid cysts can infect any organ in the body. The liver is the most common site for hydatid disease (68-80% of cases), followed by lungs (10-22.4%), spleen (0.9-8%), skeleton (0.2-3%), kidneys (0.4-3.7%), peritoneal cavity (2-5.2%), brain (0.4-1%) while aortic location is extremely location [3].
In a review of retroperitoneal cysts cases reports, 72% of patients presented with back or abdominal pain, 13,9% complained of urinary tract symptoms. 65.1% of cysts were palpable on clinical examination [4]. In general, retroperitoneal cystic lesions are uncommon and create some diagnostic difficulties and challenges in excluding a heterogeneous group of benign and neoplastic lesions in this region and consequently disease management [5].
Based on morphology, the cyst can be classified into four different types [6]:
Type 1: Simple cyst with no internal architecture.
Type 2: Cyst with daughter cysts(s) and matrix: which has three sub-types.
Type 3: Calcified cysts (dead cysts).
Type 4: Complicated cysts. eg.: ruptured cysts.
According to WHO guidelines, the first treatment option for echinococcusis is surgery. Other options include PAIR technique (puncture, aspiration, injection and reaspiration) and anti-parasitic drug treatment [7].
Case presentation
55 years old male with a previous history of radical prostatic resection presented to our outpatient clinic complaining of lower back pain that radiates toward the right lower limb and grade 2b fountain intermittent claudication.
The patient was first assessed by a neurologist who requested a lumbar spine MRI. The study revealed multiple inter-vertebral herniated discs and a 52 mm size heterogeneous retroperitoneal cyst containing multiple cystic components (Figure 1).
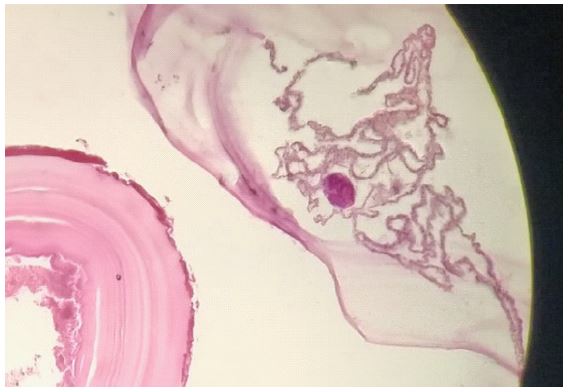
A CT guided core biopsy was done. The histological study revealed chronic inflammation, fibrosis and hyaline membranes in addition to necrotic internal germinal layer without viable scolex (Figure 2).
No anti parasitic treatment was applied. The patient was treated conservatively for the neurological and vascular complaints.
During the following period, the patient presented to the emergency department with abdominal pain and refractory vomiting not responding to conservative therapy. The clinical examination revealed tenderness, absent left femoral pulse, right iliac fossa bruit and weak right femoral pulse. Radiological study revealed small bowel obstruction. The patient underwent exploratory laparotomy, which revealed adhesion of the third duodenal segment to infra renal aortic aneurysmal dilation just above the aortic bifurcation. A gastro-jeujunal anastomosis was performed. Three weeks later, the patient underwent multi-slice computed tomography, which revealed, total occlusion of the left common iliac artery and severe stenosis of the common right iliac artery (Figure 3).


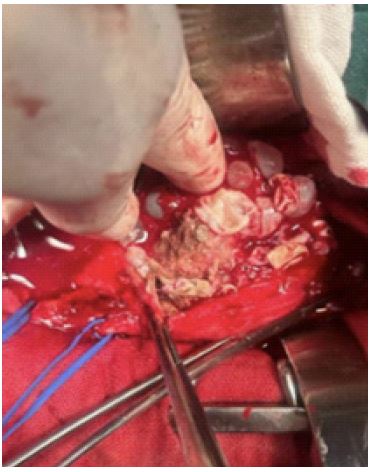
A thorough cardiac and anesthesiological work up was done to prepare the patient for open surgery. Via midline incision and trans-peritoneal approach, after careful isolation of the third duodenal segment, the infra renal aorta and common iliac arteries were well dissected and totally resected with the daughter cysts (Figures 4A and 4B). The abdomen was washed with hypertonic saline solution. The vascular axis was reconstructed by aorto-bi-iliac bypass using 16/8 mm-bifurcated collagen impregnated dacron graft. Post-surgical serological tests remained negative but albendazole therapy was applied two weeks later. Post-surgical follow up was normal.

Discussion
Hydatid cysts are infections caused by a parasite called echinococcus granulosus [1]. It usually infects lungs and liver in more than 90% of cases, while the aortic localization is usually very rare [3]. Many factors are responsible for the rarity of these cases, mainly the anatomical structure and the complex vasa vasorum, which makes the aortic wall less likely to be infected in comparison to other parenchymal organs. Additionally, the aortic wall composition of smooth muscles and connective tissue gives the parasite a harsh environment [8].
There are multiple mechanisms of aortic involvement by hydatid cysts including primary intra-mural formation, arterial wall erosion by scolex passing into the vasa vasorum through an intimal defect and adjacent cysts rupture into the vessel wall. These intramural aortic hydatid cysts might lead to catastrophic complications such as pseudo-aneurysm formation, aortic occlusion with subsequent ischemia, vertebral erosion [9] and peripheral emboli [10].
CT and MRI can show the vascular involvement and exact anatomical location of the aneurysm sac and the nature of the internal and external structures of an associated hydatid cyst. Angiography is the best technique define the communication between the aortic lumen and the cyst [11]. Serological tests, like ELISA are mandatory in assessing any patient with aortic sacular aneurysm, especially patients coming from endemic areas [10].
The preferred therapeutic approach is the open surgical one to ensure the precise and complete removal of the cyst, and the reconstruction of the aortic axis by graft interposition. Endovascular treatment was suggested, when anatomically feasible, might be a protective bridging therapy to avoid anaphylaxis, aortic rupture and systemic dissemination of the disease [11]. The pharmacological therapy with albendazole seems to play a role in minimizing the relapse risk [7].
On a literature review, valeria silvestri and colleagues found 9 cases of aortic hydatidosis. Of these cases, one case involved the abdominal aorta, one case involved the ascending aorta and arch and the remainder involved the descending thoracic aorta. The clinical presentation was chronic pain in 6 cases, acute limb ischemia in 1 case, acute neurological symptoms in 1 case involving the ascending aorta and aortic arch and subacute pain in one case. The treatment was surgical in the majority of cases and endovascular in 2 cases. No deaths were reported. Complications included one endograft stenosis and 2 cases of vertebral erosion [9].
Conclusion
In conclusion, hydatid cysts are very frequent in poor and rural areas. Liver and lungs represent the most organs infected. The vascular localizations are very rare, and they must be taken in consideration in case of para-aortic cystic lesions. Imaging modalities such as multi-slice computed tomography with 3d reconstruction and MRI can provide more detailed assessment of the relationship between the cyst and adjacent structures. Digital Subtraction Arteriography (D.S.A.) remains the best technique to study the connection between cystic cavity and aortic lumen. Serological tests, including Enzyme-Linked Immunosorbent Assays (ELISA), can help the diagnostic process by confirming the infection by ecchinococcus granulosus. Surgical resection and vascular axis reconstruction is the only treatment option which can be preceded, in some case, by endovascular stent graft bridging.
References
- Wang N, Zhong X, Song X, et al. Molecular and biochemical characterization of calmodulin from echinococcus granulosus. Parasit vectors. 2017; 10: 597.
- https://emedicine.medscape.com/article/178648-overview?src=mbl_msp_android&ref=share
- Salamone G, Licari L, Randisi B, Falcon N, Tutino R, et al. Uncommon localizations of hydatid cysts. Review of the literature. G Chir. 2016; 37: 180-185.
- Akbulut S, Senol A, Ekin A, Bakir S, Bayan K, et al. primary retroperitoneal hydatid cysts: Report of 2 cases and review of 41 published cases. Int Surg. 2010; 95: 189-196.
- Moroti A, Busso M, Consiglio Barozzino M, Cinardo P, Angelino V, et al. detection and management of retroperitoneal cystic lesions: A case report and review of the literature. Oncol Lett. 2017; 14: 1608-1608.
- Gaillard F, Ranchod A, El-Feky M, et al. Hydatid disease. 2023.
- Guidelines for treatment of cystic and alveolar echinococcois. WHO informal working group on echinococcosis. Bull World Health Organization. 1996; 74: 241-42.
- Taxifulati N, Yang XA, Zhang XF, Aini A, Abulizi A, et al. Multiple recurrent cystic echinococcosis with abdominal aortic involvement: A case report. World J Clin Cases. 2020; 8: 3108-3113.
- http://www.sciencedirect.com/science/articles/abs/pii/S1477893922002228
- Dar AM. Hydatid embolism from a thoracic aortic pseudoaneurysm presenting as gangrenous toes. 2010; 344-7.
- Volpe P, Dalainas I, Ruggieri M, Nano G, Paroni G, Rotondo G. Endovascular treatment of the descending thoracic aorta in a patient with a hydatid pseudoaneurysm. 2006; 2000-3.