
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Cutaneous squamous cell carcinoma with osteoclast-like giant cells in an 87-year-old male
Abigail Hunter1; Jarett Casale1; Bray Aron2; Natalie Depcik-Smith1,3; Ryan Geist4*
1Campbell University, Sampson Regional Medical Center, Clinton, NC, USA.
2Edward Via College of Osteopathic Medicine, Auburn, AL, USA.
3Aurora Diagnostics, Greensboro, NC, USA.
4DO 4743 Oyster Reef Run, Wilmington, NC82405, USA.
*Corresponding Author : Ryan Geist
DO 4743 Oyster Reef Run, Wilmington, NC82405, USA.
Tel: (208) 420-3436;
Email: rgeist@sampsonrmc.org
Received : Oct 06, 2023
Accepted : Nov 09, 2023
Published : Nov 16, 2023
Archived : www.jcimcr.org
Copyright : © Geist R (2023).
Abstract
Cutaneous Squamous Cell Carcinoma (SCC) with Osteoclast-Like Giant Cells (OLGCs) is a rare finding, with only 11 previous cases reported in the literature. The origin of the OLGC within carcinomas has been debated, and there are two prevailing theories regarding the cell origin. We report the 12th case of SCC with OLGCs, discuss the two theories, and analyze the common features among all twelve cases. Ultimately, there appears to be an association between OLGCs and poorly differentiated cutaneous squamous cell carcinomas. Consequently, OLGCs should lead to an increased index of suspicion, as they may be a predictor of poor outcomes. If OLGCs are identified on histology, the pathologist should consider the addition of Preferentially-expressed Antigen in Melanoma (PRAME) immunostaining as a means of more accurately determining the prognosis. In conjunction with clinical features, histology should guide clinical recommendations and may warrant chemoprevention with systemic retinoids in high-risk individuals.
Keywords: Osteoclast giant cells; Osteoclast-like giant cells; Squamous cell carcinoma; Histiocytes; cd68; p63; Cytokeratin 5; Cytokeratin 6; Immunostaining; Poorly differentiated; Retinoid.
Abbreviations: SCC: Squamous Cell Carcinoma; OLGCS: Osteoclast-like Giant Cells; PRAME: Preferentially Expressed Antigen in Melanoma; H&E: Hematoxylin and Eosin; CK 5/6: Cytokeratin 5 & 6; CD68: Cluster of Differentiation 68; P63: Tumor Protein 63.
Citation: Hunter A, Casale J, Aron B, Depcik-Smith N, Geist R. Cutaneous squamous cell carcinoma with osteoclast-like giant cells in an 87-year-old male. J Clin Images Med Case Rep. 2023; 4(11): 2694.
Introduction
Cutaneous Squamous Cell Carcinoma (SCC) with Osteoclast-Like Giant Cells (OLGCs) present on histology is a rare diagnosis with only 11 cases reported in the literature [1]. In 1968 OLGCs were first reported in association with pancreatic carcinoma and have been noted in various visceral malignancies since [2]. However, it was not until 2007 that OLGCs were first noted in cutaneous squamous cell carcinoma [3]. The origin of the OLGC with in carcinomas has been debated, and there are two prevailing theories as to where these cells originate. The first theory suggests they are tumor cells that have transformed into an osteoclast-like phenotype. This idea stems from a study of OLGCs that were in liver and pancreas tumors. In this study, they found that OLGCs and dysplastic ductal epithelial cells shared a similar mutation in K-ras suggesting the two cell types share a common progenitor [4]. The second theory proposes that OLGCs are reactive histiocytes rather than neoplastic cells and stems from studies of OLGCs in various tumors, including the pancreas, lung, and liver. In these studies, OLGCs were found to express CD68, a mesenchymal marker, which is a common but non-specific marker of histiocytes [5]. The OLGCs, in our case, also demonstrate CD68 staining, which favors the second theory of origin. Despite the origin of these cells, recognizing the rare association of OLGCs within the entity of carcinomas is important as they are difficult to diagnose histologically and may affect prognosis [6].
Case report
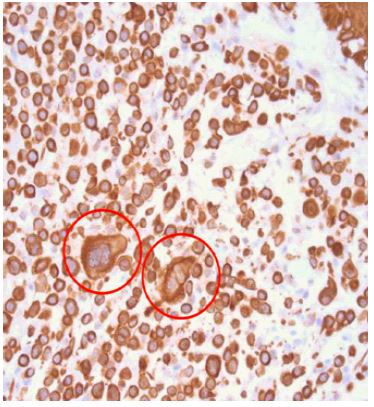
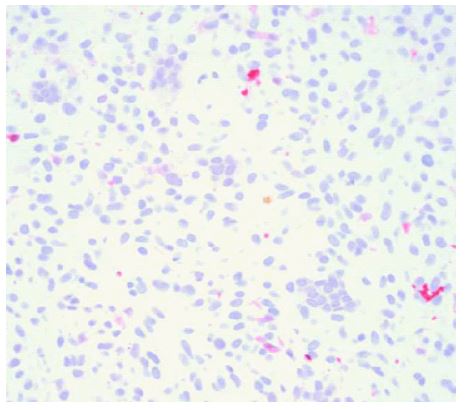
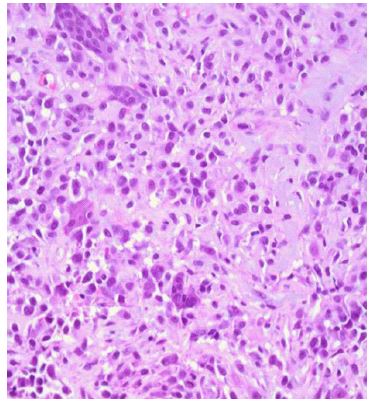
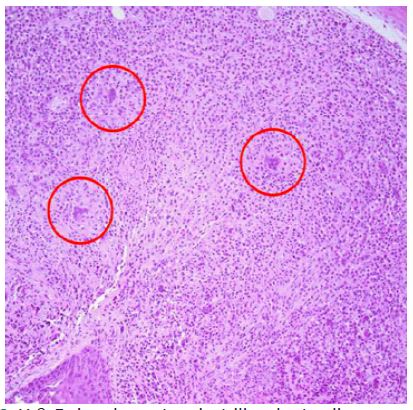
An 87-year-old male with a history of non-melanoma skin cancer presented with a 7 mm flesh-colored, crusted papule on the left central frontal scalp (Figure 1). The lesion was shave biopsied, with histological findings showing a proliferation of markedly atypical epithelial cells with evidence of squamous differentiation infiltrating the dermis on H&E. Osteoclast-type giant cells were also noted to be scattered throughout the tumor. Immunohistochemical staining for CK 5/6 and p63 highlighted the neoplastic cells, while the osteoclast-like giant cells stained positive for CD68 and negative for the cytokeratin and p63 stains. Immunohistochemical stains were performed to rule out a melanocytic lesion, including S-100 and Melan-A, which were negative. A PRAME stain was also performed and found to highlight the neoplastic cells. The staining pattern led to the diagnosis of poorly differentiated squamous cell carcinoma with osteoclast-like giant cells extending to the base of the biopsy (Figures 2-7).



Discussion
Histologically squamous cell carcinoma may present with many phenotypes, and the presence of OLGCs is a rare phenomenon. Our case demonstrated a poorly differentiated squamous cell carcinoma with OLGCs interspersed within the tumor on H&E. This diagnosis was supported by positive CK 5/6 and p63 staining of the neoplastic cells. Conversely, the OLGCs did not stain for CK 5/6 or p63 but did stain positive for CD68. This staining pattern proves the epithelial origin of the neoplastic cells and suggests that the OLGCs are of a different cellular lineage. CD68 is reactive in virtually all cells of monocyte lineage and supports the notion that the OLGCs are a histiocytic immune response to the squamous cell carcinoma rather than part of the primary neoplastic process. Furthermore, the OLGCs do not demonstrate nuclear atypia or mitoses, which favors a reactive process.
Most of the reported squamous cell carcinomas with OLGCs are associated with high-risk features, including size greater than 2 centimeters, moderate-to-poor differentiation, recurrence, and metastatic spread, which are associated with poor prognosis [1,7]. Our case did demonstrate poor differentiation and positive immunohistochemical staining with PRAME. Although commonly used as a nuclear stain formelanoma, it has been demonstrated that PRAME will stain squamous cell carcinomas and other non-melanoma cutaneous carcinomas and structures at low levels [8]. Additionally, when positive in malignant tumors, PRAME is associated with poor prognosis [8]. As such, positive PRAME staining in conjunction with the presence of OLGCs in cutaneous squamous cell carcinomas may be used to prognosticate a poor outcome. However, none of the previously reported cases of cutaneous squamous cell carcinoma with OLGCs report on the use of PRAME immunostaining, so it is unknown if this correlation would be found in a majority of cases.
Due to the tendency for squamous cell carcinoma with OLGCs to be poorly differentiated and often a high-grade neoplasm, it can be difficult to diagnose properly [1]. There are 2 cases in the literature of squamous cell carcinoma with OLGCs being misdiagnosed as atypical fibroxanthoma [9]. After re-examination of immunohistochemistry stains, it was found that the tumor cells stained weakly for pan-cytokeratin with sparing of the OLGCs. When OLGCs are visualized on Hematoxylin and Eosin (H&E) staining, it is imperative to consider the diagnosis of poorly differentiated cutaneous squamous cell carcinoma in the differential and utilize a range of cytokeratin stains to differentiate this entity from atypical fibroxanthoma. In addition, it is important to consider that cutaneous squamous cell carcinomas with OLGCs have been reported in different morphological patterns. One previously reported case in the literature found OLGCs to be juxtaposed to the body of the carcinoma as opposed to these cells being interspersed throughout the tumor, as was observed in our case [6].
Our case contributes to the theory that most cutaneous squamous cell carcinomas with OLGCs demonstrate them secondary to reactive phenomenon. Of the twelve cases reported of this histologic variant, most are found in sun-exposed and sun-damaged areas, particularly in the head and neck of males. Although it is possible that OLGCs could originate from the primary neoplastic process, the staining patterns and banality of cells in all reported cases favor a reactive occurrence. In cases with poorly differentiated cells and OLGCs, it is imperative to have a high index of suspicion for poorly differentiated cutaneous squamous cell carcinoma. OLGCs are a predictor of poor outcomes, and the addition of PRAME immunostaining and other clinical features can help develop a prognosis for the case, as well as guide clinical recommendations for chemoprevention with systemic retinoids in high-risk individuals.
Declarations
Financial disclosures: None to report.
Support: None to report.
Ethical approval: The research project was submitted for expedited review and approved by the East Alabama Medical Center Institutional Review Board.
Informed consent: Signed consent was obtained from the patient for approval of the writing and publication of this case.
Author contributions: Abigail Hunter, Jarett Casale, Ryan Geist, Bray Aron, and Natalie Depcik-Smith provided substantial contributions to conception and design of this report, acquisition of data, and the analysis and interpretation of data and drafted the article or revised it critically for important intellectual content; all authors gave final approval of the version of the article to be published and agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Acknowledgments: This research was supported (in whole or in part) by Campbell University, Sampson Regional Medical Center or Aurora Diagnostics. The views expressed in this publication represent those of the author(s) and do not necessarily represent the official views of Campbell University, Sampson Regional Medical Center or Aurora Diagnostics or its affiliated entities. This case report has not been previously presented.
References
- Venning VL, Myint E, Pyne J, et al. Poorly differentiated cutaneous squamous cell carcinoma with osteoclast-like giant cell: A rare, aggressive variant. Clin Case Rep. 2019; 7: 340-342.
- Rosai J. Carcinoma of pancreas simulating giant cell tumor of bone. Electron microscopic evidence of its acinar origin. Cancer. 1968; 22: 333-344.
- Emanuel PO, Shim H, Phelps RG. (Poorly differentiated squamous cell carcinoma with osteoclastic giant cell like proliferation. Journal of cutaneous pathology. 2007; 34: 930–933.
- Leung, KM, Wong S, Chow TC, et al. A malignant gastrointestinal stromal tumor with osteoclast-like giant cells. Archives of pathology & laboratory medicine (1976). 2002; 126: 972–974.
- Al-Brahim N, Salama S. Malignant melanoma with osteoclast-like giant cells : An unusual host response : Immunohistochemical and ultrastructural study of three cases and literature review. The American journal of dermatopathology. 2005; 27: 126–129.
- Wooff J, Werner D, Murphy J, et al. Osteoclast-Like Giant Cell Reaction Associated With Cutaneous Squamous Cell Carcinoma: A Report of 2 Cases and Review of the Literature. The American journal of dermatopathology. 2009; 31: 282–287.
- Chung, HJ, Wolpowitz D, Scott G, et al. Squamous cell carcinoma with osteoclast-like giant cells: A morphologically heterologous group including carcinosarcoma and squamous cell carcinoma with stromal changes. Journal of Cutaneous Pathology. 2015; 43: 148–157. https://doi.org/10.1111/cup.12607
- Ng, JKM, Choi PCL, Chow C, et al. PRAME immunostain expression in sebaceous lesions, cutaneous carcinomas and adnexal structures. Pathology. 2022.
- Beer TW. Squamous Cell Carcinoma With Osteoclast-Like Giant Cells: 2 Cases Misdiagnosed as Atypical Fibroxanthoma. Am J Dermatopathol. 2010; 32: 414-415.