
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Series - Open Access, Volume 4
Dendriform pulmonary ossification associated with severe SARS-CoV-2 pneumonia
Valentina Munera1; Juan F Vélez2*; Daniel Quintero3; Ana Maria Alvarado4; Jorge Carrillo5
1Radiologist, Universidad Pontifica Bolivariana, Medellin, Colombia.
2Radiology Resident, Universidad Nacional, Bógota, Colombia.
3Radiologist, Universidad Pontifica Bolivariana, Medellin, Colombia.
4Radiologist, RIMAB, Bógota, Colombia.
5Radiologist, Universidad Nacional, RIMAB, Bógota, Colombia.
*Corresponding Author : Juan Felipe Vélez
Radiology Resident, Universidad Nacional, Calle 26# 38a-11 Bogotá, Colombia.
Tel: +573137795401;
Email: juvelezj@unal.edu.co
Received : Oct 14, 2023
Accepted : Nov 13, 2023
Published : Nov 20, 2023
Archived : www.jcimcr.org
Copyright : © Vélez JF (2023).
Abstract
Dendriform pulmonary ossification is an uncommon entity in which there is metaplastic bone formation in the lungs. Cicatricial organizing pneumonia has been described as one of its causes. We present the case of four patients who developed dendriform pulmonary ossification after having severe SARS-CoV-2 pneumonia.
Keywords: Heterotopic ossification; SARS-CoV-2; Viral pneumonia; Cryptogenic organizing pneumonia; Multidetector computed tomography.
Citation: Munera V, Vélez JF, Quintero D, Maria Alvarado A, Carrillo J. Dendriform pulmonary ossification associated with severe SARS-CoV-2 pneumonia. J Clin Images Med Case Rep. 2023; 4(11): 2697.
Introduction
Dendriform pulmonary ossification may present in different forms such as idiopathic or related to illnesses of multiple natures (Chronic obstructive pulmonary disease, idiopathic pulmonary fibrosis, etc). It also manifests due to the destruction of the tunica media of arteries, followed by inflammation and hyalinization of perivascular tissue.
The lung response to SARS-CoV-2 infections is diverse and includes patterns of Diffuse Alveolar Damage (DAD), Organizing Pneumonia (OP), and Acute Fibrinous Organizing Pneumonia (AFOP). Garcia et al. [1] described a patient with dendriform pulmonary ossification after SARS-CoV-2 pneumonia. The authors hypothesize that the ossification is related to scars from organizing pneumonia, fibrous changes, and secondary bone metaplasia.
We present the cases of four patients with radiological manifestations compatible with dendriform pulmonary ossification whose only relevant clinical history was severe SARS-CoV-2 pneumonia.
Case 1
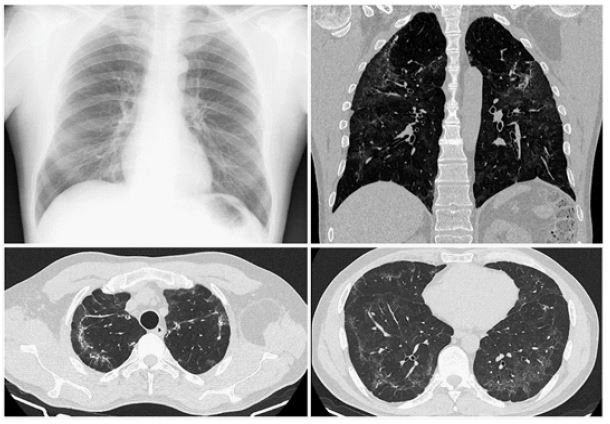
A 57-year-old male with a history of gastric neoplasm presented with 1 week of dyspnea, fever, and parenchymal opacities on X-rays. Polymerase chain reaction confirmed SARS-CoV-2 infection. The patient progressed with hypoxemic respiratory failure which required orotracheal intubation, and invasive mechanical ventilation. The persistence of parenchymal opacities in imaging studies suggested patterns of OP associated with viral pneumonia. The findings in a follow-up chest CT six months later were suggestive of dendriform pulmonary ossification.
Lung CT (Figure 1). Subpleural glass ground opacities, parenchymal bands, and apical subpleural lines with calcium density.
Case 2
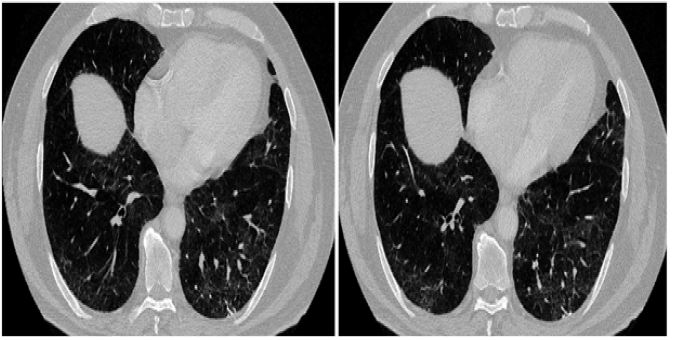
A 73-year-old male presented with 14 days of asthenia, anosmia, fever, and cough. The patient was isolated at home and a SARS-CoV-2 infection was confirmed with PCR. He developed severe hypoxemia, elevated lactate dehydrogenase, and increased D dimer. Chest X-ray showed multilobar parenchymal opacities, predominantly subpleural. The patient was treated with supplementary oxygen. A follow-up CT was performed 5 months later due to persistent dyspnea. Its findings were consistent with dendriform pulmonary ossification.
Lung CT (Figure 2). Linear densities with calcium attenuation values in both inferior lobes, subpleural glass ground opacities, parenchymal bands, and micronodules.
Case 3
A 75-year-old male with a history of arterial hypertension presented with 12 days of fever, cough, and mild dyspnea. A PCR confirmed SARS-CoV-2 infection. The patient then deteriorated and presented acute respiratory failure which required invasive mechanical ventilation in the intensive care. Chest X-ray revealed multilobar parenchymal opacities, predominating in the peripheral region. Due to persisting chest pain, a follow-up CT was performed 5 months later with linear calcifications in the lung parenchyma.
Lung CT (Figure 3). Subpleural and basal glass ground opacities, parenchymal bands, linear calcifications with apical and basal subpleural micronodules.
Case 4
A 74-year-old male with a history of atrial fibrillation, presented with acute odynophagia and cough. He presented to the emergency department due to desaturation. SARS-CoV-2 infection diagnosis was made with PCR. The patient developed respiratory failure and was admitted to the intensive care unit. A CT scan 4 months later showed parenchymal findings compatible with organizing pneumonia and dendriform pulmonary ossification.
Lung CT and MIP (Figure 4). Parenchymal bands, distorted architecture, traction bronchiectasis, calcified micronodules, and calcified lineal bands in inferior lobes with predilection to the subpleural region.
The alterations observed in the high-resolution computed tomography of the four patients were similar, including parenchymal bands, distortion of lung architecture, traction bronchiectasis, branched linear calcium densities, and calcifications (micronodules, linear branched densities). The four patients developed severe pneumonia which required mechanical ventilation in three of the patients and high flow oxygen device in the remaining one. The follow-up CT scans were performed due to persistent dyspnea in all the patients and non-specific chest pain in two of the patients. Two of the patients had prior chest X-rays from before their illness, in which opacities in lung parenchyma were not present. A checklist was employed with the goal of ruling out any other cause of lung calcifications.
Table 1: Risk factors for OPD.
| Chronic kidney disease or hemodialysis Liver transplant Primary hyperparathyroidism Administration of exogenous calcium or vitamin D History of malignancy (multiple myeloma, lymphoma, leukemia, squamouscell carcinoma, breast cancer, choriocarcinoma) Histoplasmosis, coccidioidomycosis, tuberculosis, sarcoidosis Parasitic infections Amyloidosis Silicosis Pneumoconiosis Idiopathic pulmonary fibrosis Mitral stenosis, chronic left heart failure, aortic stenosis |

Discussion
The lung response to a viral infection has previously been described and includes necrotizing bronchitis, bronchiolitis, OP, AFOP, and patterns of DAD [2]. Inflammatory response patterns have been described as part of the natural course of SARS-CoV-2 pneumonia which encompasses DAD, OP, and AFOP. These response patterns are not exclusive to viral pneumonia and are associated with different conditions or infectious organisms (bacteria and fungi), connective tissue diseases, extrapulmonary sepsis, adverse drug reactions, aspiration, collagenosis, bone marrow transplant, radiotherapy, vasculitis, and interstitial pneumonia [3].
OP is a histological pattern in which deposits of fibroblastic granulated tissue or Masson bodies are found in the alveolar sacs and ducts. It is a common response to lung damage and has a wide range of clinical and radiological manifestations. The term secondary OP is used when there is an associated cause or etiology, when no other association can be established the term cryptogenic organizing pneumonia is used [4].
The cicatricial variant of OP (COP) is a recently introduced pathological concept that refers to mixed fibrous material deposit in the bronchioles and alveolar sacs (characteristic of OP), associated with progressive fibrosis with the formation of intraluminal eosinophilic tissue without destruction of lung parenchyma [5,6]. Patches of mixed fibrous connective tissue in bronchioles and alveolar sacs can be observed in the histopathological study, with intraluminal collagen deposits, and the development of fibrous nodules or dense fibrous linear fibrotic bands, that can represent diffuse sites of ossification which can be observed in HRCT [5-7]. This variant may also have bone metaplasia, which preludes pulmonary ossification. In the cases previously presented it manifested as a dendriform pattern in imaging studies [5].
The most common representation of OP in imaging studies consists of areas of migratory consolidations and peripheral ground glass opacities. Less common radiological findings include nodules, masses, reticular opacities, reverse halo sign, and bronchiectasis [4]. Reported CT findings of COP described in the literature are peripheral consolidations, glass ground opacities, or solitary nodules [3], persistent linear opacities, and dendriform pulmonary ossification [5].
OP patterns have been found in patients with SARS-CoV-2 pneumonia which in certain cases can be associated with severe pneumonia, Adult Respiratory Distress Syndrome (ARDS), and DAD [8]. Garcia et al. described a patient who developed a dendriform pulmonary ossification pattern after having SARS-CoV-2 pneumonia. The authors postulated the presence of ossification in this patient was related to the development of cicatricial OP, with fibrous changes, and secondary bone metaplasia [1]. Recently Gallo et al. reported another case of pulmonary ossifications after COVID-19 pneumonia in a patient with a history of chronic kidney disease, hemodialysis, and secondary metabolic disorders of calcium and phosphorous metabolism. They proposed that the pulmonary tissue altered by the viral infection facilitates calcification, however, a dendriform pattern was not described in that report [9].
Dendriform Pulmonary Ossification (DPO) is uncommon and is characterized by the formation of metaplastic bone in lung parenchyma [10]. Differing from pulmonary calcifications in which only calcium salt deposits are observed, the ossification also implies the presence of an extracellular matrix, as well as the transformation of fibroblasts into osteoblasts, mediated by inflammatory factors, in an ideal biochemical microenvironment, with or without bone marrow elements [11].
Two patterns of pulmonary ossification have been described: Nodular, and dendriform. Nodular ossification has been described in association with pulmonary venous congestion, mitral stenosis, chronic left-sided heart failure, or subaortic stenosis. The dendriform pattern can be idiopathic or associated with chronic inflammation of the parenchyma, and other secondary disorders [8,11]. The secondary disorders associated with pulmonary ossification include pulmonary fibrosis, chronic obstructive pulmonary disease (COPD) ARDS, OP pattern, pneumoconiosis, asbestosis, drug-induced alveolar damage, and alveolar hemorrhage [10,12].
The precise physiological mechanisms for these pulmonary response patterns towards different noxa including viral infections are still unknown. Inflammation appears to be a determining factor for developing dendriform pulmonary ossification because it favors bone metaplasia. A microenvironment that favors an alkaline pH, and specific ionic charges, also plays an important role for the process to occur. Alterations in serum calcium, phosphorus, and alkaline phosphatase levels must be absent [11]. A greater incidence of heterotopic ossification in soft tissues has been described in musculoskeletal systems after a SARS-CoV-2 infection, especially in severe cases. Hence inflammation and local acid-base disbalances after prolonged periods of hypoxia are the most probable mechanisms [13].
The DPO findings in CT include subpleural micronodules ranging from 1-3 mm, linear ramified densities in the affected areas, without distortion of lung architecture, traction bronchiectasis, or honeycomb, and less frequently high attenuation nodules [14]. The differential diagnosis for OPD is vast and includes calcifications due to pulmonary alveolar microlithiasis, primary and secondary hyperthyroidism, severe chickenpox pneumonia, and granulomatous diseases such as tuberculosis and histoplasmosis [11].
The diagnosis in the cases presented was reached based on radiological findings, and a careful revision of the patients’ clinical history which allowed to rule out other conditions that could possibly cause DPO. None of the patients received hemodialysis previously nor presented with chronic renal disease. None of the patients were reported to have endocrinological disorders, metabolic disorders, or previous pulmonary inflammatory conditions that could explain secondary causes of OPD other than severe pneumonia from SARS-CoV-2. Further studies are needed to understand the exact mechanisms and causality of cicatricial organizing pneumonia and dendriform pulmonary ossification.
Declarations
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
- García Moreno B, Buitrago Weiland G, Sánchez Alegre M, Vanegas Rodríguez J. Accelerated Pulmonary Ossification as a Sequela of SARS-CoV-2 Pneumonia. Radiol. Cardiothorac. Imaging 2021; 3: e200598.
- Franquet T. Imaging of Pulmonary Viral Pneumonia. Radiol. 2011; 260: 18-39.
- Vadász I, Husain-Syed F, Dorfmüller P, et al. Severe organising pneumonia following COVID-19. Thorax. 2020; 76: 201-204.
- Kligerman S, Franks T, Galvin J. From the Radiologic Pathology Archives: Organization and Fibrosis as a Response to Lung Injury in Diffuse Alveolar Damage, Organizing Pneumonia, and Acute Fibrinous and Organizing Pneumonia. RadioGraphics. 2013; 33: 1951-1975.
- Yousem S. Cicatricial variant of cryptogenic organizing pneumonia. Hum Pathol. 2017; 64: 76-82.
- Bin Saeedan M, Farver C, Mehta A, Yadav R. Cicatricial Organizing Pneumonia with Dendriform Pulmonary Ossification: An Unusual Cause for a Recurrent Pneumothorax. Case Rep Pulmonol. 2019; 2019: 1-5.
- Woge M, Ryu J, Bartholmai B, Yi E. Cicatricial organizing pneumonia: a clinicopathologic and radiologic study on a cohort diagnosed by surgical lung biopsy at a single institution. Hum Pathol. 2020; 101: 58-63.
- Kory P, Kanne J. SARS-CoV-2 organising pneumonia: ‘Has there been a widespread failure to identify and treat this prevalent condition in COVID-19?’. BMJ Open Respir Res. 2020; 7: e000724.
- Gallo González V, López-Padilla D, Puente Maestú L. Calcificaciones pulmonares como secuela de neumonía COVID-19. Arch Bronconeumol. 2022; 58: 257.
- Gao Y, Egan A, Moua T. Dendriform pulmonary ossification complicated by recurrent spontaneous pneumothorax: Two case reports and a review of the literature. Respir Med Case Rep. 2020; 30: 101067.
- Chan E, Morales D, Welsh C, McDermott M, Schwarz M. Calcium Deposition with or without Bone Formation in the Lung. Am J Respir Crit Care Med. 2002; 165: 1654-1669.
- Yamagishi T, Fujimoto N, Miyamoto Y, et al. The Rapid Appearance and Disappearance of Dendriform Pulmonary Ossification after Diffuse Alveolar Hemorrhage. Am J Respir Crit Care Med. 2016; 193: 333-334.
- Meyer C, Haustrate M, Nisolle J, Deltombe T. Heterotopic ossification in COVID-19: A series of 4 cases. Ann Phys Rehabil Med. 2020; 63: 565-567.
- Gruden J, Green D, Legasto A, Jensen E, Panse P. Dendriform Pulmonary Ossification in the Absence of Usual Interstitial Pneumonia: CT Features and Possible Association With Recurrent Acid Aspiration. AJR Am. J. Roentgenol. 2017; 209: 1209-1215.