
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Complete heart block and covid19- Is there a missed connection?
Deepanjan Bhattacharya1*; Koyel Chakraborty2; Basudev Bhattacharjee1; Ajay Gautam1
1Senior Consultant, BR Singh Hospital and Centre for Medical Education and Research, Kolkata, India.
2Senior Resident, Regional Institute of Ophthalmology, Kolkata, India.
*Corresponding Author : Deepanjan Bhattacharya
Senior Consultant, BR Singh Hospital and Centre for Medical Education and Research, Kolkata, India.
Email: b.deepanjan@yahoo.co.in
Received : Oct 21, 2023
Accepted : Nov 15, 2023
Published : Nov 22, 2023
Archived : www.jcimcr.org
Copyright : © Bhattacharya D (2023).
Abstract
Tachy and bradyarrhythmias are reported complications of COVID19 infection. We report two adults with COVID19 infection induced complete heart block, with previously documented normal electrocardiogram.
Citation: Bhattacharya D, Chakraborty K, Bhattacharjee B, Gautam A. Complete heart block and covid19- Is there a missed connection?. J Clin Images Med Case Rep. 2023; 4(11): 2703.
Introduction
Although the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) predominantly affects the respiratory system, cardiac involvement is also seen in a large number of patients [1]. Arrhythmia is seen in about 44% of cases, while sinus bradycardia and atrioventricular block is seen in about 25% [2]. Although the etiopathogenesis is not clear, proposed mechanisms include a proinflammatory state arising from cytokine storm and virus-related myocardial injury [3].
We report two patients with new onset complete heart block arising from COVID19 infection.
Case 1
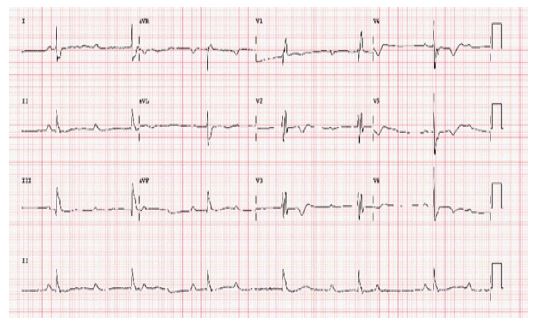
A 61-year old gentleman, with no known comorbidities presented with two episodes of syncope in one day. On examination, he had bradycardia with pulse rate of 42/min, blood pressure of 110/70 mmHg and systemic saturation of 97%, with unremarkable systemic examination. Electrocardiogram showed complete heart block, and echocardiogram showed normal biventricular systolic and diastolic function. Previous ECG done 3 months back was unremarkable. Complete blood count, serum electrolytes, thyroid profile, renal function and cardiac biomarkers were normal. Nasopharyngeal swab was positive for COVID19 RT-PCR. He was vaccinated with 2 doses of Covishield, and chest X ray was normal.
He underwent VVI pacemaker and had an uneventful stay in the hospital. At 6 months follow-up, he remains asymptomatic and completely pacing dependent.
Case 2
A 42-year old gentleman, with previously documented normal ECG, presented with sudden onset dizziness. On examination, he had bradycardia with pulse rate of 40/min, blood pressure of 120/80 mmHg and systemic saturation of 97%, with unremarkable systemic examination. Electrocardiogram showed complete heart block, and echocardiogram showed normal biventricular systolic and diastolic function. Complete blood count, serum electrolytes, thyroid profile, renal function and cardiac biomarkers were normal. Nasopharyngeal swab was positive for COVID-19 RT-PCR. He was vaccinated with 2 doses of Covishield, and chest X ray was normal.
He underwent VVI pacemaker and had an uneventful stay in the hospital. After 3 months of follow-up, he remains asymptomatic and completely pacing dependent.

Discussion
Complete AV block can be caused by increased vagal tone, cardiac conduction system disease (fibrosis), ischemic heart disease, cardiomyopathies (including sarcoidosis, hemochromatosis, or amyloidosis), infection (such as Lyme or viral myocarditis), hyperkalemia, thyroid disease, medications (including beta-blockers, calcium channel blockers, digoxin, adenosine, and antiarrhythmic medications), and post-operative complications [4].
Although no clear mechanism has been described so far in literature, direct viral infiltration of cardiomyocytes through the angiotensin-converting enzyme-2 receptors with perturbation of the cardiac conduction system is a possible explanation [5].
Although in previously reported cases [4,6,7], patients with COVID19 infection who had complete heart block had stormy in-hospital course with features of cytokine storm and high mortality, our patients were relatively asymptomatic with normal cardiac biomarker levels. However, they remained pacing dependent even on follow-up which excludes transientness of the disease.
Conclusion
COVID-19 infection can be an important cause of complete heart block even in asymptomatic patients, and always needs to be ruled out. Although the mechanism is not clear, direct infiltration by the virus may be a plausible cause.
References
- Azevedo RB, Botelho BG, Hollanda JV, et al. COVID-19 and the cardiovascular system: A comprehensive review. J Hum Hypertens. 2021; 35: 4-11.
- Kochav SM, Coromilas E, Nalbandian A, et al. Cardiac arrhythmias in COVID-19 infection. Circ Arrhythm Electrophysiol. 2020; 13.
- Manolis AS, Manolis AA, Manolis TA, Apostolopoulos EJ, Papatheou D, et al. COVID-19 infection and cardiac arrhythmias. Trends Cardiovasc Med. 2020; 30: 451-460.
- Bassi R, Ismail Z, Salabei JK, Charles K, Haider AA, et al. COVID-19-Induced Complete Heart Block: Case Series and Literature Review. Cureus. 2023; 15: e37517.
- Salabei JK, Asnake ZT, Ismail ZH, et al. COVID-19 and the cardiovascular system: An update. Am J Med Sci. 2022; 364: 139-147.
- El-Assaad I, Hood-Pishchany MI, Kheir J, et al. Complete heart block, severe ventricular dysfunction, and myocardial inflammation in a Child with COVID-19 infection. JACC Case Rep. 2020; 2: 1351-1355.
- Kavya NP, Sudan A, Patel NB, Panda PK. Complete heart block in COVID-19 without prior cardiac disease. J Family Med Prim Care. 2022; 11: 4851-4853.