
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Congenital hyperextension of the knee without dislocation in a child: A case report
Paul Mutani1*; George Constantine1; Caroline Maxwell1,2; John Changalucha1; Saidi Kapiga1,2; Kathy Baisley2;
Deborah Watson-Jones1,2; Charles J Lacey3
1Mwanza Intervention Trials Unit, National Institute for Medical Research, Mwanza, Tanzania.
2London School of Hygiene & Tropical Medicine, Keppel Street, London, United Kingdom.
3York Biomedical Research Institute, Hull York Medical School, University of York, York, United Kingdom.
*Corresponding Author : Paul Mutani
Mwanza Intervention Trials Unit/National Institute for Medical Research, PO. BOX 11936, Mwanza, Tanzania.
Tel: +255-28-2500019; +255758929200;
+255-28-2542162
Email: mutanipaul@yahoo.com;
mutani.mwanagindu@mitu.or.tz
Received : Oct 21, 2023
Accepted : Nov 18, 2023
Published : Nov 25, 2023
Archived : www.jcimcr.org
Copyright : © Mutani P (2023).
Abstract
Congenital hyperextension of the knee, also known as congenital genu recurvatum, is a rare medical condition with an incidence of 1:100,000 deliveries. It is typically diagnosed clinically at birth, aided by radiological findings. Treatment with serial casting and close follow-up has been demonstrated to provide most favourable results.
A Tanzanian 15-years-old primigravid girl with a normal gynaecological history was enrolled into a clinical trial evaluating the immunogenicity of different doses of two human papillomavirus vaccines (clinicaltrials.gov identifier NCT02834637). Fifty-five weeks after she received the second dose of the bivalent vaccine, Cervarix®, she delivered a female infant by spontaneous vaginal delivery following normal labour, at an estimated gestational age of 41 weeks. The infant had a notable right knee deformity but was otherwise well. Five days later, the baby was examined at the research clinic and noted to have a right knee hyperextension with limited flexion. X- rays reviewed by a consultant orthopaedic surgeon revealed congenital hyperextension of the right knee without dislocation. The baby girl recovered fully after three months of serial casting.
We report a rare case of congenital hyperextension of the right knee without dislocation that recovered fully after serial casting and close follow up in a girl participating in a HPV vaccine trial. The anomaly was considered to be unrelated to the vaccine.
Keywords: Congenital hyperextension; Cervarix®; Case report.
Citation: Mutani P, Constantine G, Maxwell C, Changalucha J, Kapiga S, et al. Congenital hyperextension of the knee without dislocation in a child: A case report. J Clin Images Med Case Rep. 2023; 4(11): 2704.
Introduction
We report a case of congenital hyperextension of the knee also known as congenital genu recurvatum, a rare congenital malformation of the knee with the estimated incidence of 1:100,000 deliveries. It is characterized by abnormal hyperextension of one or both knees with limited flexion with or without dislocation of the knee joint [1,2,4-8]. Just as in our case report, there is female predominance and the unilateral right knee involvement is not uncommon as compared to left and bilateral knee involvement [9,10-17]. It may either occur as an isolated birth defect or it may be associated with other musculoskeletal anomalies such as developmental dysplasia of the hip and clubfoot, or it may occur as part of a syndrome such as arthrogryposis multiplex congenita or Larsen syndrome, or it may be associated with neurologic disorder such as meningomyelocele [3].
There is no specific aetiology that is known but there are existing known predisposing factors which are either intrinsic or extrinsic. The intrinsic factors are mainly genetic and commonly associated with specific disorders such as larsen syndrome, Arthrogryposis, Achondroplasia, and/or neuromuscular imbalances. The extrinsic factors include conditions that increase intrauterine pressure leading to mal-positioning of the joints, decrease in utero space such as in oligohydramnios, traumatic dislocation of the joints during the birthing process, umbilical cord entanglement especially around the legs, mal-positioning of the uterus and breech presentation [8-13].
Patient information
A teenage girl, participant of the HPV vaccine trial (Dose Reduction Immunobridging and Safety study of two Human Papillomavirus (HPV) vaccines among Tanzanian girls-DoRIS) which is evaluating the safety and immunogenicity of a single dose of HPV vaccines versus two and three doses was enrolled and randomized to receive two doses of a bivalent (HPV 16/18) HPV vaccine, Cervarix®. Her second vaccination happened four months before she reported her last normal menstrual period. Her pregnancy was confirmed at the research clinic by a positive urine pregnancy test at the estimated gestational age of 38 weeks.
She delivered a baby girl at the gestational age of approximately 41 weeks at a nearby health facility. Baby was delivered by spontaneous vaginal delivery, with body weight of 3.1 kgs and apgar score of 7/10. Labour was normal and there was no breech presentation. Immediately after delivery, the midwives informed the baby’s mother that her baby had a right knee abnormality.
She had an uneventful gynaecological history and neither had she had any history of chronic diseases nor congenital anomalies in the family. Also, she had no history of cigarette, alcohol or illicit drug use and her nutritional status was normal.
Plaster of Paris (POP) cast was applied on the new-born’s deformed knee few hours later.
Clinical findings
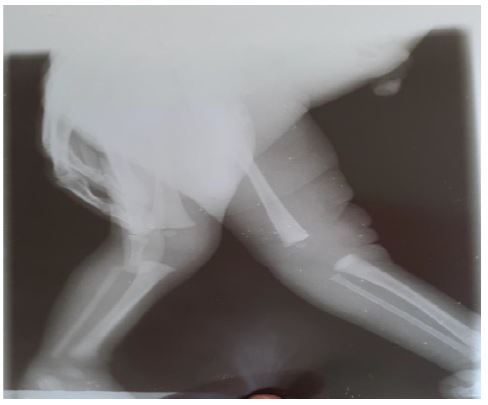
Baby was reviewed at the research clinic five days after delivery; upon examination, she was found to have a swollen right knee which was mildly tender with limited flexion and over extension as shown in the images (Figure 1: Photos at five days old initial photos). Lateral X ray view of the right knee revealed posterior knee joint dislocation as interpreted by the consultant orthopaedic surgeon, Sekou Toure Regional Referral Hospital, Mwanza who also recommended continuation of the application of POP as shown in the Figure 1.
Diagnostic assessment and therapeutic intervention
We conducted another review at the research clinic a month later while also being supported by the consultation from the orthopaedic surgeon; the baby’s knee showed significant progress, swelling and pain had subsided, the knee was able to flex without limitations and the knee joint was stabilizing.
We reached for expert opinion from the consultant orthopaedic surgeon, Great Ormond Street Hospital, London and he suggested that the baby girl has a congenital hyperextension of the right knee without dislocation and recommended continuation of the POP application and periodic follow up.
Follow-up and outcomes
The baby was again followed up for review a month later (two months postdelivery) and displayed significant improvement through marked reduction of swelling and tenderness as well as reduction of limitation on range of movement of the right knee.
Three months post delivery, follow up at the Regional Referral Hospital revealed marked improvement, baby had no complaints, no swelling and no tenderness was noted on the right knee, she was able to flex and extend the knee without limitations as illustrated in images (Figure 2: Photos at three months old-Follow up photos). The local orthopaedic surgeons considered that the baby had recovered fully, POP cast was removed and no further follow up was recommended.



Discussion
Congenital hyperextension of the knee is classified according to the grade of tibiofibular anterior displacement and also alternatively classified according to the degree of knee flexion. Grade 1 is mainly when there is only hyperextension of the knee, Grade 2 is when there is hyperextension of the knee with anterior subluxation of the tibia and fibula and Grade 3 is when there is hyperextension with anterior dislocation of the knee and fibula [11]. Based on the range of passive knee flexion, Grade 1 is when knee flexion is greater than 90⁰, Grade 2 30-90⁰, and Grade 3 being less than 30⁰ [9].
Diagnosis of this condition is made through clinical examination and radiological findings of the knees at birth in the delivery room or might be made antenatally by ultrasonography [18]. Clinical diagnosis requires assessment of the degree of hyperextension and palpation of the femoral condyles, which become more prominent as the severity of the hyperextension increases [10]. X rays or ultrasound will support the diagnosis by helping to assess whether a true dislocation or subluxation of the tibia on the femur has occurred [13,18].
Management of this condition and the outcome of the treatment largely depends on whether the child has other congenital anomalies or whether the birth defect is a part of other rare congenital abnormalities such as Larsen syndrome, arthrogryposis or achondroplasia. Mostly the greater part of the treatment is serial casting and tractions, surgery is only applicable when these methods have unfavourable outcomes. Studies have stipulated that treatment initiated as early as 8 hours after delivery has good prognosis [7].
It is highly unlikely that our patient’s diagnosis was the result of the extrinsic factors since her mother had normal labour with neither breech presentation nor umbilical entanglement. We did not have access to whole genome sequencing to investigate possible mutations. We also classified our case as Grade 1 since there was only hyperextension of the knee with neither subluxation or dislocation of the knee joint.
Our patient’s mother is a recipient of a bivalent HPV vaccine, which she was given two doses as a participant in the DoRIS trial and reported to have conceived four months after receiving the last vaccine dose. Given the interval between last vaccination and conception, we do not think there is any relation between vaccination and the occurrence of this rare disease condition. Moreover, there is no data which has shown a relation between HPV vaccine with congenital anomalies [15,16].
Because the baby’s mother was participating in a clinical trial, this case was categorised as a Serious Adverse Event (SAE) according to Guideline for Good Clinical Practise ICH E6 (R2) [14], and reported to both the ethics committees in Tanzania and the London School of Hygiene and Tropical Medicine, UK, and the regulatory authority, the Tanzania Medicines and Medical Devises Authority (TMDA) according to the trial protocol. It was judged that it was not related with either the Cervarix® vaccine or clinical trial procedures.
Our child neither had other congenital anomalies nor any other associated bone abnormalities indicating the conservative treatment option with serial casting and close follow up and bearing favourable results. The treatment started as early as few hours after birth (within the first 12 hours of birth) and lasted for three months when the last review was conducted and determined that the child had recovered fully. The study team followed up the child until when it was determined that the girl has fully recovered and wrote a final SAE report according to the trial protocol. The child received good quality care including consultation from consultant Orthopaedic surgeons from within and outside the country. This was most likely due to the participation of the mother in the DoRIS trial.
Conclusion
Congenital hyperextension of the knee in our case was managed conservatively through serial casting and close follow up. The notable good prognosis in this case was associated with early application of POP cast that was done few hours after birth and was continued up to three months. We recommend that POP cast application as early as the first 12 hours of life and close follow up should be the mainstay of the management of children with congenital hyperextension of the knee without dislocation.
Also, lack of temporal association between vaccination and conception, we do not think there is relationship between exposure to a bivalent HPV vaccine and congenital hyperextension of the knee. However, more data on congenital hyperextension of the knee occurring in individuals who have received HPV vaccination should be analysed to confirm or refute our conclusion.
Declarations
Ethical approval and consent to participate: The authors are accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. All procedures performed in this study (DoRIS trial from which this case report was written) were in accordance with the ethical standards of the Tanzania National Institute for Medical Research, United Kingdom London School of Hygiene and Tropical Medicine and Tanzania Medicine and Medical Devices Authority and with the Helsinki Declaration (as revised in 2013).
Consent for publication: Written informed consent was obtained from the patient’s parent (mother of the patient) for publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal.
Availability of data and materials: All data, images and any other patient information in this case report is available in the data storage section of the Mwanza Intervention Trials Unit- National Institute for Medical Research Mwanza Centre and is currently not publicly available. Other information referenced in this case report is available in the internet and can be accessed.
Competing interests: The authors declare that there were no competing interests in this case report.
Funding: DoRIS trial from which this case report was written is funded by the UK Department for International Development (DFID)/MRC/Wellcome Trust Joint Global Health Trials Scheme (MR/N006135/1) and the Bill and Melinda Gates Foundation (OPP1167526). The funders of the trial did not have any role in the design of this case report, data collection and analysis, data interpretation or writing of this report.
Authors contributions: PM prepared, organized and coordinated the manuscript, GC, CM, SK, JC, KB, DW, CL contributed in writing the manuscript. All authors read and approved the final manuscript.
Acknowledgement: Authors wish to express their gratitude to all those who participated in gathering data that supported the preparation of this paper. This includes the DoRIS study staff at Mwanza Intervention Trials Unit/Tanzania National Institute for Medical Research- Mwanza Centre, Labour ward nurses as well as the Radiology staff at the Sekou Toure Regional Referral Hospital and the national and external consultant orthopaedic surgeons for providing the diagnostic support.
References
- Cashman JP, Round J, Taylor G, et al. The natural history of developmental dysplasia of the hip after early supervised treatment in the Pavlik harness. A prospective, longitudinal follow-up. J Bone Joint Surg Br. 2002; 84: 418-425
- Mehrafshan M, Wicart P, Ramanoudjame M, et al. Congenital dislocation of the knee at birth- part 1: clinical signs and classification. Orthop Traumatol Surg Res. 2016; 102: 631-633.
- Abdelaziz TH, Samir S. Congenital dislocation of the knee: A protocol for management based on degree of knee flexion. J Child Orthop. 2011; 5: 143-149.
- Elmadağ M, Ceylan HH, Imren Y, et al. Congenital dislocation of knee. Eur J Gen Med. 2013; 10: 164-166.
- Katz MP, Grogono BJ, Soper KC. The etiology and treatment of congenital dislocation of the knee. J Bone Joint Surg Br. 1967; 49: 112-120.
- Dungy CI, Leupp M. Congenital hyperextension of the knees in twins. Clin Pediatr (Phila). 1984; 23: 169-72.
- Donaire AR, Sethuram S, Kitsos E, et al. Congenital bilateral knee hyperextension in a well-newborn infant. Res J Clin Pediatr. 2017; 1.
- Farhad T, Jan V. Unilateral congenital dislocation of the knee and hip: a case report. Acta Orthop Belg. 2012; 78: 134-138.
- Gregory OO, Effiong AJ, Ebegi AI, et al. Congenital knee dislocation: Challenges in management in a low resource center. IOSR JDMS. 2016; 15: 78-82.
- Tiwari M, Sharma N. Unilateral congenital knee and hip dislocation with bilateral clubfoot-A rare packaging disorder. Journal of orthopaedic case reports. 2013; 3: 21.
- Kalawar RP, Chaudhary S, Kalam A, et al. Congenital genu recurvatum with dislocation of knee: A case report. Journal of Nobel Medical College. 2012; 1: 68-70.
- Charif P, Reichelderfer TE. Genu recurvatum congenitum in the newborn: its incidence, course, treatment, prognosis. Clinical pediatrics. 1965; 4: 587-594.
- Dasarathy J, Adedipe A, Hawke A. Hyperextension of the bilateral knees in a 1-day old neaonate: A case report. Journal of Family Practice. 2019; 68: 4.
- Ich Harmonised Guideline: Integrated Addendum To Ich E6 (R1): Guideline For Good Clinical Practice E6 (R2) Current Step 4 version. 2016.
- Heather SL, Gabriela VB, James DN, et al. Maternal and Infant Outcomes After Human Papillomavirus Vaccination in the Periconceptional Period or During Pregnancy. Obstet Gynecol. 2017; 130: 599-608
- Anshi W, Chang L, Yunan W, et al. Pregnancy Outcomes After Human Papillomavirus Vaccination in Periconceptional Period or During Pregnancy: A Systematic Review and Meta-analysis, Human Vaccines & Immunotherapeutics. 2020; 16: 581-589.
- B Omololu, SO Ogunlade, TO Alonge. Congenital dislocation of the knee in Ibadan, Nigeria.West African Journal of Medicine. 2002; 21: 4.
- Rumyantsev NY, Kruglov IY, Omarov GG, et al. Congenital dislocation of the knee: Prenatal diagnostics and treatment at an early age. Pediatr Traumatol Orthop Reconstr Surg. 2017; 5: 26-35.